
Musicians as athletes
I affirm this with the conviction of someone who knows these two universes well: musicians are high-performance athletes, but they do not treat themselves as such. Professional musical performance and high-performance sports require very similar levels of commitment, as well as physical and mental demands. The time, commitment and consistency required to achieve a high level of performance playing an instrument or performing a specific sport skill have much more in common than one might initially think. Some differences will lie in the fact that, in general, neuromuscular recruitment associated with playing an instrument has a greater focus on fine motor skills (i.e. short movements of greater precision and performed mainly with the limbs extremities) and less at the level of gross motor skills (i.e. larger movements involving larger muscle groups) that we normally associate with sports movements. However, it should be clarified that both large muscle groups play an important role, particularly at a postural level, in instrumental performance, and the smaller muscles associated with fine motor skills also play a fundamental role in most sports movements.
For example, if we establish a parallel between playing the violin and performing a given sport specific skill in tennis, we find that, although at different levels, a balance of fine and gross motor control is necessary for better performance in both activities. When we play the violin, we want to maintain a high and controlled posture so that holding the violin with the non-dominant arm and handling the bow with the dominant arm allows the fine work of the hands and fingers to occur as efficiently as possible. Now, if the musculature involved in the stabilization of the trunk and in the elevation of the arms is weak, fatigue sets in more quickly resulting in postural loss, in an execution carried out with greater muscle tension and consequently in a worse performance. In the case of the serve in tennis, due to the high demand for motor coordination and strength involving all the large muscle groups of the lower and upper body, there is also a need for high levels of fine motor skills coordination regarding wrist, hand and finger movements, in order to implement a given spin effect and the desired direction to the ball.
In fact, both musical and sports performance involve neuromuscular recruitment to produce movement and work that requires precision, speed, endurance and strength. In addition, and particularly at a professional level, playing an instrument and playing a sport are activities that require long hours of repetitive movements that, combined with poor physical conditioning, can lead to a variety of clinical conditions. It is unthinkable that a highly competitive athlete does not follow a training program targeting the development of his/her physical qualities which should be complementary to the practice of his/her sport. It is easy to recognize that a good physical fitness level will ensure greater resilience and longevity in sports. The same applies to musical performance. Musicians are high-performance athletes and should prepare themselves as such! Living and playing with pain is not inevitable, it is an option.
The prevalence of pain and injury in musicians
As the years go by and the hours playing their instrument accumulate, it is almost inevitable that professional musicians develop musculoskeletal and/or neuromuscular problems of varying severity at some point in their career. More so if they do nothing about their physical preparation. Review studies on the prevalence of injuries in professional musicians point out that 76% of musicians suffer or have suffered from physical problems that prevent them from performing at their usual level and 84% had injuries that interfered negatively with their musical practice1. Some musicians will develop tendinopathies and low back pain of varying intensity, which they will be able to manage with chronic intake of anti-inflammatory medications or simply by playing less frequently and/or just by enduring pain and discomfort. Others will develop more serious overuse injury syndromes that will become chronic and compromise not only quality of musical performance, but also quality of life, forcing them to periods of musical inactivity. Additionally, others will suffer from even more serious forms of injury that may result in abandoning their career as an instrumentalist musician.
In general, the most frequent injuries affecting musicians manifest themselves through pain and/or dysfunction, especially on the joints, tendons, ligaments and nerves of the upper limb, head, neck and spine. For example, in orchestral instrumentalists, injuries of musculoskeletal and/or neuromuscular origin are more common and affect about 64% musicians, of which 20% consist of peripheral nervous problems and about 8% of cases of focal dystonia2. It makes sense, considering that these are the most stressed areas of the body during instrumental practice. An exception would be the cases of focal dystonia, which, although it may be accompanied by pain and musculoskeletal injury, the root cause of the dysfunction observed at the peripheral level is actually central, that is, the dysfunctional neuronal circuits are at the upper levels of the central nervous system such as the cerebral cortex. Thus, the most frequent injuries in instrumentalist musicians can be summarized as follows3:
- Musculoskeletal injuries – epicondylitis, tendinopathies (tendinosis, tendinitis, tenosynovitis), bursitis, arthritis, arthrosis, osteoarthritis, contractures, injuries to the temporomandibular joint;
- Nerve trapping and inflammation – carpal tunnel syndrome, thoracic outlet syndrome, radial tunnel syndrome, ulnar nerve compression syndrome, ulnar tunnel syndrome, cervical and lumbar radiculopathies;
- Hypermobility;
- Focal dystonia;
- Hearing loss.
The onset of injuries in musicians is due to an array of factors that naturally interact. Several authors have identified the following factors facilitating and/or causing the development of injuries in musicians1:
- Physiological and biological factors such as gender and age. Women seem to be more likely to develop peripheral musculoskeletal and nerve injuries compared to men, and individuals who engage in high volume instrumental practice at an early age, at 4-5 years of age, are also more likely to develop injuries later in life4,5. In the case of focal dystonia, there is a clear higher prevalence in males (over 90%) and in women with menstrual disorders, which suggests that hormonal factors may be predisposing to the development of this disorder6.
- Type of instrument. The characteristics of the instrument (size, shape and weight) and the time of practice imply different levels of physical demand, in which fatigue onset and an execution based on too much physical effort can lead to the development of injuries7. For example, the position needed to play the clarinet implies that the entire weight of the instrument is supported on the right thumb, and at the same time it requires a large amount of short and fast movements of the fingers of both hands8. Another example particularly special to me is the double bass. A bulky instrument with an air column of considerable inertia, which requires not only considerable grip strength to press on the strings, but also considerable whole body physical effort (which, can of course, be optimized with efficient technique) to move this column of air and make the instrument vibrate and produce sound. Anyone who has tried playing the double bass for a few minutes realizes the physical demands that playing this instrument encompasses.
- Instrumental technique. A poor instrumental technique, with non-optimized positions, based on physical effort rather than on movement efficiency, associated with long hours of practice without rest, will naturally predispose the player to pain and injury, especially in the wrists, hands, neck and shoulders9 .
- Specific technical demands. The technical demands of a particular musical piece that often requires high-speed and high-intensity execution, with fatiguing repetition of movements or maintenance of extreme hand positions for a long period of time. All of this creates high levels of mechanical stress and may cause injury10,11.
- Body asymmetry. In the same way that an athlete of a one-side dominant sport will try to compensate for these asymmetries by working out both sides of the body, a musician is in a similar situation, because playing an instrument implies asymmetrical work in very unnatural positions for long periods of time, which will favor the occurrence of various muscular imbalances12.
- Poor physical fitness. Good levels of strength and general physical conditioning are essential to maintain a good position to play an instrument for long periods of time. Most of these positions are very unnatural. Being in good physical fitness will allow to resist the onset of fatigue, recover more quickly between rehearsals or practice sessions, and in fact, it will allow to tolerate more hours of practice avoiding technique and performance deterioration7. Muscle imbalances and weakness resulting from long hours of sitting in certain positions and high volume repetition of short movements must be prevented through exercise programs aiming to strengthen the body globally, and at the same time to compensate for muscle imbalances induced by instrumental practice13.
- Other lifestyle factors. We know that lifestyle factors such as smoking or smoke exposure, alcohol consumption, sleep deprivation, malnutrition, poor hydration and obesity have very damaging effects at a systemic level on our body. Regarding neuromuscular injuries, we know that all these forms of toxicity weaken the body’s connective tissue (cartilage, tendons, ligaments, membranes), muscles and nerve conduction, predisposing to the development of localized inflammatory processes as well as chronic injuries. For example, did you know that obesity is highly predisposing to development of carpal tunnel syndrome?14 Or that smoking is strongly associated with development of injuries and dysfunctions in the shoulder?15
Preventing and resolving injuries in musicians
Any elite athlete empirically knows something that has long been supported by science. That the most effective way to prevent (and also treat) overuse or overload injuries due to high volume sports practice is to ensure good levels of physical fitness combined with good recovery habits, adequate rest and nutrition. Regarding physical fitness, it is unthinkable for an elite athlete, not to follow a regular physical training program. An athlete knows that this will have negative consequences both on sports performance and on the susceptibility for developing injuries. The athlete knows that the weaker his/her musculoskeletal system is, the greater the vulnerability to injury. The question is, and if we consider that professional musicians are required to engage on activities requiring high physical and mental performance for long hours of daily practice, shouldn’t musicians treat themselves as high-performance athletes? I am certain that they should.
In fact, a 2019 systematic review investigating the topic of physical training for professional orchestra musicians1 indicates that following a structured physical training program of varying durations (from a few weeks to several months) has generally resulted in significant improvements in musical performance and in reducing (and even eliminating) chronic pain1.
To keep playing at the highest level for a long time, musicians would greatly benefit if they treated themselves as high-performance athletes and ensure that they maintain good physical shape combined with good habits of recovery, rest and nutrition. And to be clear, when I talk about staying in good physical shape, I don’t mean playing sports. In fact, playing sports as a mean to improve one’s physical fitness is not ideal and can even be harmful. More activity with asymmetric characteristics would be added on top of another, also asymmetric, which is playing a musical instrument. In general, all sports are constituted by specialized movements, and for that reason, also asymmetrical. So, except for purely recreational reasons (which can also be positive at a mental and stress release level), the practice of a sport as a strategy to improve physical fitness is not ideal and should not be the first choice particularly by musicians (I discuss this very topic in this article: Why musicians should not play sports).
General physical fitness is improved through the process of training our physical qualities. This should entail an assessment of the initial status in order to identify specific limitations and outline a specific intervention strategy. One should always start at the base and progress from there, just like the process of learning to play a musical instrument. Here, attention to detail is key. A well-designed training program implies the management of training variables specific to the profile and objectives of the athlete or, in this case, the musician. A correct selection of exercises is crucial, as well as close monitoring of their implementation regarding form of execution, training load and progression over time. As I mentioned, it is not very different from the process of learning to play a musical instrument!
For a musician, playing the instrument is the top priority. It can be obsessive, I know. But playing better in the long run does not necessarily mean playing more hours, but rather investing in taking care of the ‘’machine’’ that is our body. I reiterate once more that playing with pain or discomfort is an option and not an inevitability. Take care of your body and treat it well, because you will need it in the long run!
Train well to play well!
Nuno Correia
References:
- Gallego, C., Ros, C., Ruíz, L., Martín, J. (2019). The physical training for musicians. Systematic review. Sportis Sci J, 5 (3), 532-561.
- Lederman, R. J. (2003). Neuromuscular and musculoskeletal problems in instrumental musicians. Muscle & Nerve, 27(5), 549–561.
- Betancor Almeida, I. (2011). Hábitos de actividad física en músicos de orquestas sinfónicas profesionales: un análisis empírico de ámbito internaciona Tesis Doctoral. Universidad de Las Palmas de Gran Canaria, Las Palmas de Gran Canaria.
- Fishbein, M., Middlestadt, S., Ottati, V., Straus, S., y Ellis, A. (1988). Medical problems among ICSOM musicians: Overview of a national survey. Medical Problems of Performing Artists, 3(1), 1–8.
- Viaño, J. J. (2004). Estudio de la relación entre la apariciación de lesiones musculoesqueléticas en músicos instrumentistas y hábitos de actividad física y vida diaria. En III Congreso De La Asociación Española de Ciencias Del Deporte. Valencia: Universidad de A Coruña.
- Rosset-Llobet, J., Candia, V., Fàbregas, S., Ray, W., & Pascual-Leone, A. (2007). Secondary motor disturbances in 101 patients with musician’s dystonia. Journal of neurology, neurosurgery, and psychiatry, 78(9), 949–953.
- Sardá, E. (2003). En forma: ejercicios para músicos. Barcelona: Paidos.
- Thrasher, M., y Chesky, K. (1998). Medical problems of clarinetists: Results from the U.N.T. musician health survey. The Clarinet, 25(4), 24–27.
- Wynn, C. B. (2004). Managing the physical demands of musical performance. En Williamon A. (Ed.), Musical excellence: Strategies and techniques to enhance performance (pp. 41–60). Londres: Oxford University Press.
- Bejjani, F. J., Kaye, G. M., y Benham, M. (1996). Musculoskeletal and neuromuscular conditions of instrumental musicians. Archives of Physical Medicine and Rehabilitation, 77(4), 406–413.
- Mark, T., Gary, R., y Miles, T. (2003). What every pianist needs to know about the body: a manual for players of keyboard instruments: piano, organ, digital keyboard, harpsichord, clavichord. GIA Publications. Martín.
- Ackermann, B., Adams, R., y Marshall, E. (2002). Strength of endurance training for undergraduate music majors at a university? Medical Problems of Performing Artists, 17(1), 33– 41.
- Frabretti, C., y Gomide, M. F. (2010). A saúde dos músicos: dor na prática profissional de músicos de orquestra no ABCD paulista. Revista Brasileira de Saúde Ocupacional, 35(121), 33– 40.
- Shiri R, Pourmemari MH, Falah-Hassani K, Viikari-Juntura E. The effect of excess body mass on the risk of carpal tunnel syndrome: a meta-analysis of 58 studies. Obes Rev. 2015;16(12):1094-1104.
- Bishop, Julie Y. et al. (2015). Smoking Predisposes to Rotator Cuff Pathology and Shoulder Dysfunction: A Systematic Review. Arthroscopy, Volume 31, Issue 8, 1598 – 1605.
Os músicos como atletas
Afirmo-o com a convicção de quem conhece bem estes dois universos: os músicos são atletas de alto rendimento, mas não se tratam como tal. A performance musical profissional e a performance desportiva de alto rendimento obrigam a níveis de compromisso e exigência física e mental muito semelhantes. O tempo, empenho e consistência necessários para alcançar uma performance de alto nível a tocar um instrumento ou no desempenho de um desporto específico têm muito mais em comum do que se poderia, à partida, pensar. Algumas diferenças residirão no facto de, duma forma geral, o recrutamento neuromuscular associado a tocar um instrumento ter um enfoque maior ao nível da motricidade fina (i.e. movimentos curtos de maior precisão e executados iminentemente com as extremidades) e menor ao nível da motricidade grossa (i.e. movimentos de maior amplitude envolvendo os grupos musculares de maior dimensão) que normalmente identificamos associados aos gestos desportivos. Contudo, convém esclarecer que tanto os grandes grupos musculares, como os músculos de menor dimensão associados à motricidade fina, têm uma função importante a nível postural, na execução instrumental e nos mais variados gestos desportivos.
Por exemplo, se estabelecermos um paralelismo entre tocar violino e a execução de um gesto desportivo como o serviço no ténis, verificamos que, embora a diferentes níveis de exigência, um equilíbrio do controlo motor fino e grosso é necessário para uma melhor performance em ambas as actividades. Quando tocamos violino, queremos manter uma postura alta e controlada por forma que o segurar do violino com o braço não dominante e o manejar do arco com o braço dominante, permita que o trabalho fino das mãos e dedos ocorra da forma mais eficiente possível. Ora, se a musculatura envolvida na estabilização do tronco e na elevação dos braços for fraca, a fadiga instala-se mais rapidamente resultando numa deterioração postural, numa execução em maior esforço e consequente numa pior performance. No caso do serviço do ténis, à elevada exigência de coordenação motora e força envolvendo todos os grandes grupos musculares do membro inferior e superior, junta-se a necessidade de coordenação fina ao nível dos movimentos do pulso, mão e dedos, por forma a imprimir na bola o efeito e a direcção que se pretende.
De facto, tanto a performance musical como a desportiva envolvem recrutamento neuromuscular para produzir movimento e trabalho que requer precisão, velocidade, endurance e força. Além disso, e sobretudo a um nível profissional, tocar um instrumento e praticar um desporto são actividades que obrigam a longas horas de prática de gestos repetitivos que, aliado a um mau condicionamento físico, poderá conduzir a uma variedade de problemas médicos. É impensável que um atleta de alta competição não siga um programa de treino das qualidades físicas complementar à prática do seu desporto. É fácil de entender que é uma boa condição física de base que irá garantir maior resiliência e longevidade na prática desportiva. O mesmo se aplica à performance musical. Os músicos são atletas de alta competição e deverão preparar-se como tal! Viver e tocar com dor não é uma inevitabilidade, é uma opção.
A prevalência de dor e lesões nos músicos
À medida que os anos passam e as horas agarrados ao instrumento se acumulam, é quase inevitável que os músicos profissionais desenvolvam em determinado momento da sua carreira problemas musculoesqueléticos e/ou neuromusculares de gravidade variável. Isto se não fizerem nada no que concerne à sua preparação física. Estudos de revisão sobre a prevalência de lesões em músicos profissionais apontam para que 76% dos músicos sofrem ou sofreram de problemas físicos que os impedem de actuar ao seu nível habitual e 84% tiveram lesões que interferiram negativamente com a sua prática musical1. Alguns músicos ficar-se-ão por tendinopatias e lombalgias de intensidade variável que conseguirão gerir à custa da toma crónica de medicamentos anti-inflamatórios ou simplesmente tocando menos frequentemente e suportando dor e desconforto. Outros, desenvolverão síndromas lesionais por sobreuso mais graves que se tornarão crónicos e comprometerão não só a qualidade da performance, mas também a qualidade de vida, obrigando a períodos de inactividade musical. Outros ainda, sofrerão de formas de lesão ainda mais graves que poderão resultar no abandono da carreira como músico instrumentista.
De uma forma geral, lesões mais frequentes em instrumentistas afectam e manifestam-se através de dor e/ou disfunção sobretudo das articulações, tendões, ligamentos e nervos do membro superior, cabeça, pescoço e coluna. Por exemplo, em instrumentistas de orquestra as lesões de origem músculo-esquelética e/ou neuromuscular são mais comuns afectando cerca de 64% dos músicos, dos quais 20% são problemas do foro nervoso periférico e cerca de 8% são casos de distonia focal2 . O que faz sentido, tendo em conta que essas são as zonas do corpo mais stressadas durante a prática instrumental. Excepção feita à distonia focal, que apesar de poder estar acompanhada de dor e lesão músculo-esquelética, a origem da disfunção observada a nível periférico é, na verdade, central, ou seja, os circuitos neuronais disfuncionais estão comprometidos logo nos níveis superiores do sistema nevoso central como o córtex cerebral. Assim, as lesões mais frequentes em músicos instrumentistas podem ser resumidas da seguinte forma3:
- Lesões músculo-esqueléticas – epicondilite, tendinopatias (tendinose, tendinite, tenossinovite), bursite, artrite, artrose, osteoartrite, contracturas, lesões na articulação temporomandibular;
- Bloqueio e inflamação nervosa – síndroma do túnel cárpico, síndroma do desfiladeiro torácico, síndroma do túnel radial, síndroma de compressão do nervo ulnar, síndroma do túnel ulnar, radiculopatias cervicais e lombares;
- Hipermobilidade;
- Distonia focal;
- Perda de audição.
O surgimento de lesões nos músicos deve-se a um conjunto de factores que, naturalmente, interagem. Vários autores identificaram os seguintes factores como facilitadores e/ou provocadores do surgimento de lesões nos músicos1:
- Factores fisiológicos e biológicos como género e idade. As mulheres instrumentistas parecem ter maior propensão para desenvolver lesões músculo-esqueléticas e nervosas periféricas em relação aos homens, e indivíduos que iniciem precocemente a prática instrumental com elevado volume, aos 4-5 anos de idade, também têm maior probabilidade de desenvolver lesões mais tarde na sua carreira4,5. No caso da distonia focal há uma prevalência clara no sexo masculino (acima de 90%) e em mulheres com distúrbios menstruais, o que sugere que factores hormonais podem ser predisponentes para o desenvolvimento desta patologia6.
- O tipo de instrumento. As características do instrumento (tamanho, forma e peso) e o tempo de prática implicam níveis diferentes de exigência física, em que a fadiga instalada e a execução em esforço podem levar ao desenvolvimento de lesões7. Por exemplo, a posição inerente a tocar clarinete implica que todo o peso do instrumento esteja suportado sobre o polegar direito, e ao mesmo tempo requer uma grande quantidade de movimentos curtos e rápidos dos dedos de ambas as mãos8. Outro exemplo que me diz especial respeito, é o contrabaixo de cordas. Um instrumento volumoso com uma coluna de ar de inércia considerável, que requer não só considerável força de preensão da mão que pisa as cordas, como um esforço físico (que na verdade se quer minimizar em favor de uma técnica de execução o mais eficiente possível) para fazer movimentar essa coluna de ar e fazer o instrumento vibrar e produzir som. Quem já experimentou tocar contrabaixo alguns minutos percebe bem a dimensão física que o instrumento poderá ter.
- Técnica instrumental. Uma técnica de instrumento débil, com posições não optimizadas, mais baseada em esforço físico do que numa técnica eficiente, associada a longas horas de prática sem descanso, vai naturalmente predispor o instrumentista à dor e à lesão sobretudo nos pulsos, mãos, pescoço e ombro9.
- A exigência performativa. A exigência técnica de uma determinada peça musical que muitas vezes requer uma execução a elevada velocidade, elevada intensidade, com fatigante repetição de movimentos ou manutenção de posições extremas das mãos durante um largo período de tempo. Tudo isto é gerador de stress mecânico e poderá ser causador de lesão 10,11.
- Assimetria corporal. Da mesma forma que um atleta de modalidades com enfoque unilateral irá tentar compensar essas assimetrias trabalhando os dois lados do corpo, um músico encontra-se numa situação semelhante, pois tocar um instrumento implica um trabalho assimétrico em posições muito pouco naturais por longos períodos de tempo, favorecendo a instalação de vários desequilíbrios musculares12.
- Má condição física. Bons níveis de força e uma boa condição geral é essencial para manter uma boa posição ao tocar um instrumento durante longos períodos de tempo. Posições essas, na sua maioria, muito pouco naturais. A melhoria da condição física irá permitir resistir ao instalar da fadiga, recuperar mais rapidamente entre ensaios ou sessões de estudo, e na verdade, irá permitir tolerar mais horas de prática sem deterioração da técnica musical e performance7. Desequilíbrios e fraqueza musculares resultante das longas horas sentado, da manutenção de certas posições e da repetição exaustiva de movimentos curtos devem ser tratados através de programas de treino que incluam exercícios que fortaleçam o corpo de forma global e que, ao mesmo tempo, visem compensar desequilíbrios musculares específicos induzidos pela prática instrumental13.
- Outros factores de estilo de vida. Sabemos que aspectos do estilo de vida como fumar ou exposição ao fumo, consumo de álcool, privação de sono, má nutrição, má hidratação e obesidade têm efeitos muito nefastos a nível sistémico no nosso corpo. No que concerne ao desenvolvimento de lesões do foro neuromuscular, sabemos que todas estas formas de toxicidade fragilizam todo o tecido conjuntivo (cartilagem, tendões, ligamentos, membranas), os músculos e a condução nervosa, predispondo à ocorrência de processos inflamatórios localizados e ao desenvolvimento de lesões crónicas. Sabia que, por exemplo, a obesidade predispõe grandemente para o desenvolvimento da síndrome do túnel cárpico?14 Ou que fumar está fortemente associado ao desenvolvimento de lesões e disfunções no ombro?15
Prevenir e resolver lesões nos músicos
Qualquer atleta de elite sabe empiricamente algo que há muito tempo é corroborado pela ciência. Que a forma mais eficaz de prevenir (e também curar) lesões de sobreuso ou sobrecarga devido à prática desportiva com elevado volume é garantir uma boa condição física de base aliada a bons hábitos de recuperação, descanso e nutrição. No que concerne à sua condição física, não passa pela cabeça de um atleta de elite, não seguir um programa regular de desenvolvimento das qualidades físicas. Ele sabe que isso terá consequências negativas quer no seu rendimento desportivo, quer na sua susceptibilidade para desenvolver lesões. Ele sente na pele que quanto mais fraco o seu sistema músculo-esquelético se encontrar, mais susceptível estará de se lesionar devido ao elevado volume a que a sua prática desportiva de alta performance obriga. A pergunta que se impõe é, e se considerarmos que a actividade em que os músicos profissionais incorrem constitui uma actividade de alta performance física e mental que obriga a largas horas de prática diária, não deverão os músicos tratar-se como atletas de alto rendimento? Eu tenho a certeza que sim.
De facto, numa revisão sistemática de 2019 sobre treino físico para músicos profissionais de orquestra1, os autores indicam que seguir um programa de treino físico estruturado de durações variadas (desde algumas semanas a vários meses), resultou, de uma forma geral, em melhorias significativas na performance e na redução (e mesmo eliminação) de dores crónicas.
Para manter-se a tocar ao mais alto nível e por muito tempo, os músicos beneficiariam muito se se tratassem como atletas de alto rendimento. Garantir que se mantêm em boa forma física conjugado com bons hábitos de recuperação, descanso e nutrição. E atenção, quando falo em manter-se em boa forma física não me refiro a praticar desporto. Aliás, praticar desporto como forma de melhorar a condição física não é ideal e até pode ser prejudicial. Pois estar-se-á a adicionar mais uma actividade com características assimétricas a outra também ela assimétrica que é tocar um instrumento musical. Em geral, todos os desportos são por definição constituídos por movimentos especializados, e por isso mesmo, assimétricos. Por isso, a não ser por razões meramente lúdicas (que também pode ser positivo a um nível mental), a prática de um desporto como estratégia para melhorar a condição física não é ideal e não deve ser a forma escolhida em especial pelos músicos (abordo esta questão neste artigo: Porque é que os músicos não devem fazer desporto?).
A condição física geral de base melhora-se através do treino das qualidades físicas. Isto pressupõe uma avaliação da situação inicial para aferir as limitações específicas e delinear uma estratégia de intervenção. Há que começar sempre pela base e progredir a partir daí, tal como o processo de aprender a tocar um instrumento musical. Aqui, a atenção ao detalhe é fundamental. Uma estratégia bem delineada implica uma gestão das variáveis do treino específica para a condição e objectivos do atleta ou, neste caso, do músico. É crucial uma correcta selecção de exercícios, e monitorização de perto da sua implementação quanto à forma de execução, carga utilizada e progressão ao longo do tempo. Como referi, não é muito diferente do processo de aprender a tocar um instrumento musical!
Para um músico, tocar o instrumento é a prioridade das prioridades. Pode ser obsessivo, eu sei. Mas tocar melhor e no longo prazo não passa necessariamente por tocar mais horas, mas por investir em cuidar da ‘’máquina’’ que é o nosso corpo. Volto a reforçar que tocar com dor ou desconforto é uma opção e não uma inevitabilidade. Cuidem do vosso corpo e tratem-no bem, pois irão precisar dele no longo prazo!
Bons ensaios e bons treinos!
Nuno Correia
Referências:
- Gallego, C., Ros, C., Ruíz, L., Martín, J. (2019). The physical training for musicians. Systematic review. Sportis Sci J, 5 (3), 532-561.
- Lederman, R. J. (2003). Neuromuscular and musculoskeletal problems in instrumental musicians. Muscle & Nerve, 27(5), 549–561.
- Betancor Almeida, I. (2011). Hábitos de actividad física en músicos de orquestas sinfónicas profesionales: un análisis empírico de ámbito internaciona Tesis Doctoral. Universidad de Las Palmas de Gran Canaria, Las Palmas de Gran Canaria.
- Fishbein, M., Middlestadt, S., Ottati, V., Straus, S., y Ellis, A. (1988). Medical problems among ICSOM musicians: Overview of a national survey. Medical Problems of Performing Artists, 3(1), 1–8.
- Viaño, J. J. (2004). Estudio de la relación entre la apariciación de lesiones musculoesqueléticas en músicos instrumentistas y hábitos de actividad física y vida diaria. En III Congreso De La Asociación Española de Ciencias Del Deporte. Valencia: Universidad de A Coruña.
- Rosset-Llobet, J., Candia, V., Fàbregas, S., Ray, W., & Pascual-Leone, A. (2007). Secondary motor disturbances in 101 patients with musician’s dystonia. Journal of neurology, neurosurgery, and psychiatry, 78(9), 949–953.
- Sardá, E. (2003). En forma: ejercicios para músicos. Barcelona: Paidos.
- Thrasher, M., y Chesky, K. (1998). Medical problems of clarinetists: Results from the U.N.T. musician health survey. The Clarinet, 25(4), 24–27.
- Wynn, C. B. (2004). Managing the physical demands of musical performance. En Williamon A. (Ed.), Musical excellence: Strategies and techniques to enhance performance (pp. 41–60). Londres: Oxford University Press.
- Bejjani, F. J., Kaye, G. M., y Benham, M. (1996). Musculoskeletal and neuromuscular conditions of instrumental musicians. Archives of Physical Medicine and Rehabilitation, 77(4), 406–413.
- Mark, T., Gary, R., y Miles, T. (2003). What every pianist needs to know about the body: a manual for players of keyboard instruments: piano, organ, digital keyboard, harpsichord, clavichord. GIA Publications. Martín.
- Ackermann, B., Adams, R., y Marshall, E. (2002). Strength of endurance training for undergraduate music majors at a university? Medical Problems of Performing Artists, 17(1), 33– 41.
- Frabretti, C., y Gomide, M. F. (2010). A saúde dos músicos: dor na prática profissional de músicos de orquestra no ABCD paulista. Revista Brasileira de Saúde Ocupacional, 35(121), 33– 40.
- Shiri R, Pourmemari MH, Falah-Hassani K, Viikari-Juntura E. The effect of excess body mass on the risk of carpal tunnel syndrome: a meta-analysis of 58 studies. Obes Rev. 2015;16(12):1094-1104.
- Bishop, Julie Y. et al. (2015). Smoking Predisposes to Rotator Cuff Pathology and Shoulder Dysfunction: A Systematic Review. Arthroscopy, Volume 31, Issue 8, 1598 – 1605.

Após as últimas semanas de isolamento que vivemos, prepara-se agora gradualmente o regresso à normalidade. Uma normalidade que será ainda bastante diferente daquilo que conhecíamos, pedindo-se, nesta fase, que se aprenda a conviver com o vírus.
Ora bem, tendo em conta que o vírus veio para ficar e que vamos ter efetivamente de viver com ele, nunca foi tão importante cuidar da sua alimentação e estilo de vida para que o seu sistema imunitário tenha todas as ferramentas necessárias para combater este vírus de forma eficaz, caso haja um possível contágio.
Em primeiro lugar, é importante perceber, de forma muito simplista, como funciona este vírus. O SARS-CoV-2 tem a habilidade de estimular uma libertação descontrolada de citocinas pró-inflamatórias, levando a um efeito de tempestade de citocinas, causando lesão tecidual e danos graves no epitélio respiratório.
Assim sendo, parece que a palavra a reter é inflamação, sendo esta a causa dos danos graves e mesmo da morte. Extrapolando um pouco o raciocínio, quem sofre contágio com um status inflamatório mais elevado, está, à partida, em maior risco de sofrer danos mais severos. E é isso que se tem observado! As pessoas com comorbilidades, nomeadamente obesidade, doenças autoimunes, hipertensão arterial, cancros, são considerados grupos de risco para esta pandemia e possuem, também todos eles, estados inflamatórios mais acentuados.
Portanto, a chave parece ser trabalharmos nos nossos estilos de vida, para melhorarmos o nosso status inflamatório e assim diminuirmos o risco de sofrer de uma doença crónica não transmissível. Ao mesmo tempo, é importante fornecermos as ferramentas para que o nosso sistema imunitário seja capaz de uma resposta adequada em caso de contágio. Como é que isso se faz?
Em primeiro lugar, e isto é, de longe, o ponto mais importante de todo este artigo. O grande segredo, o grande milagre, a pílula mágica para melhorar a sua alimentação do dia para noite é só um, coma COMIDA! Mas comida de verdade, daquela que não tem ingredientes, nem rótulos, nem marketing ou alegações de saúde. Falo de carne, peixe, marisco, ovos, vegetais, fruta, oleaginosas. Simples assim!
Comer comida de verdade deixa-o num ponto muito mais à frente que a grande maioria das outras pessoas no que toca à capacidade de resposta do seu sistema imunitário. Isto porque, quando comemos alimentos de verdade, o seu organismo recebe uma panóplia variada de vitaminas, minerais, antioxidantes, fitoquímicos, polifenóis, tudo aquilo que o organismo necessita para funcionar de forma correta. No entanto, e tendo em conta as necessidades e os requisitos específicos de cada indivíduo, é de extrema importância a individualização, razão pela qual é essencial ser acompanhado por um profissional da área da nutrição.
Outro ponto de extrema importância e que está diretamente relacionado com o anterior: a nossa imunidade começa no intestino e, portanto, ter um microbiota diversificado e saudável e uma mucosa intestinal íntegra é essencial. Sabemos que o microbiota é um grande responsável pelo status inflamatório do organismo, sendo, portanto, de máxima importância cuidarmos das nossas bactérias intestinais.
Para tal, é essencial o consumo adequado de fibra, solúvel e insolúvel. E portanto, voltamos a falar de frutas e vegetais! Estas deverão estar presentes em grandes quantidades na dieta de todos nós. Para além da fibra, o consumo de alimentos fermentados deve ser incentivado, nomeadamente vegetais fermentados (como por exemplo chucrute), kombucha e kefir, como forma de modular o microbioma e reparar a mucosa intestinal.
Tendo em conta que o vírus SARS CoV-2 é relativamente recente, ainda não são muitos os estudos que nos mostrem quais os compostos ativos que têm uma ação direta no vírus. No entanto, conhecendo o mecanismo de atuação do SARS CoV-2, podemos aferir ou deduzir quais os compostos que vão atuar na diminuição da capacidade do vírus infetar as nossas células, diminuir a replicação viral e dar suporte ao nosso sistema imunológico.
Assim sendo, existem alguns compostos ativos, vitaminas e minerais que atuam nestas diferentes vias. Alguns destes compostos podem ser obtidos através de suplementação específica e outros através da alimentação. No entanto, é preciso relembrar que a suplementação deve ser prescrita por um profissional de saúde, tendo em conta as necessidades e o historial clínico de cada um. Não é adequado tomar suplementos sem haver um motivo clínico que o justifique.
Naturalmente que nenhum destes suplementos impede o contágio e, neste sentido, apenas as medidas de higiene adequadas e o distanciamento social são eficazes. Não obstante, em caso de contágio, o nosso sistema imunitário tem de ser o mais eficaz a combater o vírus e a diminuir os sintomas associados.
Os seguintes nutrientes e compostos ativos de forma isolada parecem ser grandes aliados:
Vitamina A: desempenha um papel importante na função imune, regulando as respostas imunes celulares e humorais (Huang et al., 2018). A nível alimentar pode ser encontrada nas vísceras dos animais, como fígado, e nas gemas dos ovos. A suplementação só deve ser considerada caso se confirmem défices a nível sérico.
Vitamina C: contribui para a defesa imunológica, melhorando a quimiotaxia e fagocitose (Beveridge, Wintergerst, Maggini and Hornig, 2008). A suplementação com vitamina C pode não ser necessária caso a ingestão alimentar seja adequada. Para isso, é necessário consumir frutas e vegetais ricos em vitamina C ao longo do dia, nomeadamente kiwis, citrinos, morangos, pimentos, agrião e salsa.
Vitamina D: participa na modulação da resposta tanto do sistema imune inato como adaptativo. Parece haver uma relação entre o status de vitamina D do indivíduo e a resposta antiviral contra infeções respiratórias (Jayawardena et al., 2020). A suplementação só deve acontecer caso existam défices, mas esta é muitas vezes necessária, especialmente durante os meses de Inverno.
Zinco: participa no funcionamento do sistema imunitário e diminui a replicação viral, reduzindo a gravidade das infeções. A deficiência de zinco está assim associada a uma maior susceptibilidade a infeções virais (Read, Obeid, Ahlenstiel and Ahlenstiel, 2019). No entanto, e uma vez mais, a suplementação só deve ser feita caso se verifiquem défices comprovados deste mineral. Na alimentação, pode ser encontrado nas ostras, na carne vermelha e nas sementes de girassol.
Selénio: possui propriedades anti-inflamatórias e um efeito antioxidante. A deficiência de selénio está associada com uma função imune mais débil (Rayman, 2012). O consumo diário de castanhas do Brasil pode auxiliar na obtenção de valores adequados de selénio no organismo.
Melatonina: tem um efeito antioxidante e anti-inflamatório e promove uma diminuição nas citocinas inflamatórias em circulação (Zhang et al., 2020). A suplementação pode ser necessária, dependendo das necessidades do indivíduo.
Estas são algumas das estratégias a aplicar em termos alimentares. No entanto é importante (re)lembrar que as mudanças a efetuar devem ser de estilo de vida, onde se devem incluir hábitos de exercício físico regular, adequação de padrões de sono, gestão de stress e diminuição da exposição a toxinas. Todas estas alterações contribuirão para a diminuição da inflamação e para melhoria da função do sistema imunitário, tão importante para os tempos actuais e para a melhoria da nossa qualidade de vida.
Andreia Luís de Castro
Referências:
Beveridge, S., Wintergerst, E., Maggini, S. and Hornig, D., 2008. Immune-enhancing role of vitamin C and zinc and effect on clinical conditions. Proceedings of the Nutrition Society, 67(OCE1).
Huang, Z., Liu, Y., Qi, G., Brand, D. and Zheng, S., 2018. Role of Vitamin A in the Immune System. Journal of Clinical Medicine, 7(9), p.258.
Jayawardena, R., Sooriyaarachchi, P., Chourdakis, M., Jeewandara, C. and Ranasinghe, P., 2020. Enhancing immunity in viral infections, with special emphasis on COVID-19: A review. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 14(4), pp.367-382.
Rayman, M., 2012. Selenium and human health. The Lancet, 379(9822), pp.1256-1268.
Read, S., Obeid, S., Ahlenstiel, C. and Ahlenstiel, G., 2019. The Role of Zinc in Antiviral Immunity. Advances in Nutrition, 10(4), pp.696-710.
Zhang, R., Wang, X., Ni, L., Di, X., Ma, B., Niu, S., Liu, C. and Reiter, R., 2020. COVID-19: Melatonin as a potential adjuvant treatment. Life Sciences, 250, p.117583.
Given the times we live in, where social contact is limited, the promotion of online services in all professional areas proliferates. In fitness, it seems that it has suddenly been discovered that you can (and should) train every day and that you can train at home and/or on your own. It is incredible the explosion of posts on social media by personal trainers offering sequences of exercises for people to perform at home. We know that, for better health and resilience, it is essential to exercise every day, just as it is essential to eat well and maintain personal hygiene, but this has always been so and, therefore, it is not only a necessity of current times.
For this reason, posting an exercise line-up for everyone to perform is as valuable as posting a photo of a meal or of someone brushing their teeth. It serves as much to remind you that these activities are important, but the content is not, to a large extent, applicable to you reading this text. Much less when it comes to exercise. In fact, picking up the fork and knife to eat, or the act of brushing your teeth are less complex activities than performing most of the physical exercises that we often see proposed, let alone organizing them in a training session.
The health and resilience resulting from training is even more relevant in times of crisis such as the one we are experiencing now, but that health and resilience was mainly built months and years prior to this moment. Notably during those months and years that you consistently went to the gym to do your workout, often with personal sacrifice. It is hard to organize oneself in order to be able to train! We have family and work and it is sometimes difficult to reconcile all social and professional obligations with the time we choose to invest in our health and well-being, like in the case of training. Notice that now I’m using the term training.
Because many of you who are reading these lines have long understood the difference between “exercising” and training. Many of you have realized that “exercising” is better than nothing, but that training is at a higher level. Training is a process that requires the organization and management of a range of variables over time. It requires making a careful assessment of the initial condition, selecting specific exercises and the ways to perform them, observing and evaluating movement, and making the necessary adjustments (e.g. load, type and form of exercise execution) in order to ensure constant progression along the path towards health, performance and resilience. Training is not the same as ‘’doing exercises” always varied and without criteria just to maintain some physical activity. And because some of you understand this difference, you have come over the months and years that preceded today’s turbulent times to make organizational sacrifices in order to train. And you chose to invest a little more of your time and money, and regularly went to a gym to get a training service. A service in which a program is followed, the exercises are not chosen at random, and in which the progression in the loads used as well as the execution of the exercises is closely monitored by a coach.
All the benefits of personalized training are possible to obtain remotely via online. I believe that the in-person format will always be superior, but with good organization and commitment from both the coach and student, constant progression is possible, and this difference can be mitigated. How do we know this at The Strength Clinic? Because we’ve been doing it for years! In addition, personalized training followed online may even have some advantages over the face-to-face format, such as:
- Not having to go to the gym at any given time. This can be a great advantage for some people. If the self-discipline of following your training program is guaranteed, travel time and what it implies in organizational terms is saved. In addition, you can choose a training time slot that best fits your schedule without being conditioned by the availability of your coach;
- Greater consistency and commitment doing the exercises in your program. Since you can choose the time slot of your training session, you are less likely to miss it, as you will have more flexibility in adjusting the schedule if needed. This way, it is more likely that you reach the weekly training frequency that is desirable. In addition, as we recommend that you document on video a summary of each workout on an online platform so that your coach can observe, this also adds an additional sense of commitment to the session and the proper execution of the exercises;
- Better cost benefit. In fact, you will be able to enjoy almost all the benefits of having a personal trainer for a lower price because you will not have to pay for the running costs of the facility and its equipment usage where the in-person training session would take place;
- Train directly with your favorite coach. If the coach you would like to work with is not available in-person or his/her in-person rate is beyond your means, the online option will allow you to work directly with him for a lower price.
The message “don’t stop training even if you are at home or on your own” in the context of the crisis we are experiencing today is correct! However, this need did not arise today. It is something that should be part of our lives if we want to remain getting stronger and healthier forever. For this purpose, training is much better than just “exercising”, especially if you follow workouts taken from social media that do not take into account your specific profile, your body awareness and do not follow any criteria for exercise selection and future programming. It only serves the purpose of “moving the body” and getting tired in that moment or day, but it will not accomplish much more than that. Because training implies a process that is based on your goals and individual characteristics. In a training session, what you do today was based on what you did yesterday and what you are going to do in the future. And it is possible to continue to train online and reap all the benefits of personalized training, even at a distance. It requires a mutual commitment of the student and coach in a process that is joint. Your optimized personal development will always be our commitment at The Strength Clinic. We are here to guide you through this process rather that offering “one size fits all” workouts for everyone!
Stay strong!
Nuno Correia

Este artigo é técnico e específico, se aquilo que pretende é apenas saber o que precisa fazer, pode ir directamente para a conclusão. Se, porventura, quiser educar-se um pouco mais sobre o potencial do exercício na sua saúde e imunidade, recomendo que vá buscar um café ou um chá e que leia o artigo completo.
Introdução
Uma das questões mais recorrentes nos últimos tempos em virtude do tema “Coronavírus” é se o exercício físico pode melhorar a função do sistema imunitário. Mas vamos recuar primeiro um pouco no tempo. A necessidade de se movimentar ou de fazer exercício para manter ou melhorar a saúde não é nova. O movimento sempre foi e sempre será uma necessidade essencial à condição humana. O problema actual é que no nosso estilo de vida moderno (altamente sedentário) a maior parte das pessoas esqueceu-se disso, deixou de alimentar a sua motricidade e pensa que consegue resolver os seus problemas de saúde com soluções rápidas ou temporárias de fitness.
Ou seja, se sabemos que o exercício tem a possibilidade de afectar todos os órgãos e sistemas do corpo humano, é natural (e desejável) que o sistema imunitário seja também regulado pelo nível de actividade física de cada indivíduo. A inactividade física em conjunto com a perda de massa muscular (e alimentação deficiente) irá facilitar a imunosenescência, a perda de função do sistema imunitário. Clinicamente, isto significa um maior risco de infecções, reactivações mais frequentes de vírus latentes, diminuição da eficácia da vacinação e aumento da prevalência de doenças auto-imunes e cancro1.
Portanto, temos por um lado o movimento ou a actividade física, que é transversal à evolução de qualquer homo sapiens e, por outro, temos o treino físico, que pode ser o catalisador para elevar os resultados da performance humana para outros patamares. A percepção geral de que a actividade física regula o sistema imunitário é correcta mas a ideia generalizada de que qualquer forma de exercício melhora o sistema imunitário é incorrecta. Simplesmente não podemos ignorar os princípios elementares da biologia humana e do ciclo de stress, recuperação e adaptação inerentes a cada indivíduo.
Contextualização da imunologia do exercício
Embora a imunologia do exercício seja considerada (relativamente) uma nova área de investigação científica, com 90% dos trabalhos publicados após 19902, alguns dos primeiros estudos foram publicados há mais de um século. Por exemplo, em 1902, Larrabee3 demonstrou que as alterações nas contagens diferenciais de glóbulos brancos nos corredores de maratona de Boston eram semelhantes às observadas em certas condições de doença, com uma “considerável leucocitose do tipo inflamatório”.
De acordo com a revisão efectuada por Nieman4, uma das maiores autoridades mundiais em imunologia do exercício, e que por acaso já correu mais de 50 maratonas, as descobertas científicas neste campo podem ser divididas em quatro períodos distintos. De 1900 a 1979, o foco era nas alterações agudas e na função das células imunitárias. De 1980 a 1989, vários estudos sugeriram que o esforço de intensidade elevada estava associado com uma disfunção imunitária transiente, com a elevação de biomarcadores inflamatórios e com um aumento do risco de infecções do trato respiratório superior. Durante o período de 1990 a 2009, foram adicionadas outras áreas complementares de estudo, incluindo o efeito interactivo da nutrição, os efeitos do exercício no envelhecimento do sistema imunitário e as influências nas citocinas inflamatórias. A partir de 2010, com os avanços na espectometria de massa e na tecnologia associada aos testes genéticos, começou-se a depositar maior atenção em áreas de estudo como a metabolómica, lipidómica, proteómica e microbioma, com o intuito de fornecer directrizes mais personalizadas ao nível da nutrição e exercício.
Portanto, já sabemos há muito tempo que o sistema imunitário é muito sensível ao exercício físico e, como tal, será a extensão e a intensidade do exercício, que vão reflectir o nível de stress fisiológico imposto ao sistema imunitário. Claramente, durações e intensidades elevadas em simultâneo não fazem bem à saúde.
O envelhecimento e o seu impacto na imunosenescência
A deterioração do sistema imunitário com a idade deve-se principalmente a factores biológicos, como a genética e às interacções com factores ambientais (como a exposição a agentes infecciosos, incluindo citomegalovírus), impondo alterações metabólicas causadas por estilos de vida não saudáveis (exercício inadequado, dieta inadequada) e stress fisiológico prolongado5,6.
A imunosenescência associada ao envelhecimento acontece pelo menos através dos seguintes três fenómenos: 1) redução na resposta imunitária; 2) aumento da inflamação e oxidação (em inglês inflammaging e oxi-inflammaging); 3) produção e libertação de auto-anticorpos.
No caso do primeiro, o envelhecimento influencia principalmente a imunidade através de alterações na estrutura e actividade do timo (i.e., atrofia do timo), uma glândula com importantes funções imunitárias localizada entre os pulmões, da redução na produção de linfócitos (linfopoiese primária)7,8, do declínio das células T ingénuas, da acumulação das células T memória e de uma diminuição na produção de anticorpos9-11. O envelhecimento também está associado ao declínio das células estaminais hematopoiéticas (hemocitoblastos) e à função das células progenitoras, resultando num aumento da produção de células da linhagem mielóide e diminuição no potencial linfóide12.
No que diz respeito ao segundo, o envelhecimento poderá contribuir para o aumento da secreção de citocinas inflamatórias (interleucina-1 [IL-1], factor de necrose tumoral alfa [TNF-α], interleucina-6 [IL-6] e proteína C reactiva [PCR])13. Com o avançar da idade, os macrófagos, que actuam como sentinelas e residem nos tecidos conjuntivos e orgãos do corpo, tornam-se mais pró-inflamatórios, libertando maiores quantidades de TNF-α e de interleucina-12 (IL-12)14, o que pode acelerar os danos nos tecidos.
Finalmente, no que concerne ao terceiro, o aumento da produção e libertação de auto-anticorpos poderá levar a um aumento de manifestações auto-imunes15,16.
Efeitos do exercício na imunosenescência
Muitos trabalhos têm demonstrado que um estilo de vida fisicamente activo pode ter efeitos positivos no envelhecimento do sistema imunitário17,18. Em particular, o exercício físico regular parece afectar os processos de envelhecimento do sistema imunitário inato (também chamado de não específico) e adaptativo (também chamado de específico ou adquirido). Por exemplo, um dos testes mais robustos para medir a competência imune é a resposta mediada por anticorpo ou célula a novos antígenos, frequentemente administrados experimentalmente por vacinação. As respostas humorais (imunidade mediada pelos linfócitos B) e celulares (imunidade mediada pelos linfócitos T) à vacinação parecem ser mais fortes nos indivíduos activos em comparação com os indivíduos sedentários e mais fortes também naqueles que realizaram formas de exercício estruturado nos meses que antecederam a administração da vacina19,20.
O exercício regular no envelhecimento parece estar associado a um melhor funcionamento das células natural killer (NK)21, a primeira classe de glóbulos brancos a actuar em resposta a qualquer vírus, bactéria ou tumor. Da mesma forma, o funcionamento dos neutrófilos parece ser afectado positivamente, uma vez que idosos saudáveis e mais activos têm uma melhor migração de neutrófilos em direcção à interleucina-8 (IL-8)22, uma citocina com efeitos na angiogénese23 (formação de novos vasos sanguíneos) e, potencialmente, no desenvolvimento muscular. As intervenções com exercício demonstraram diminuir o número de monócitos inflamatórios circulantes CD16+24 (o termo CD significa “cluster of differentiation” e surgiu como forma de diferenciar as diferentes classes de células imunológicas) e a melhorar a função dos neutrófilos e a fagocitose em pacientes com artrite reumatóide25.
Estudos transversais antigos em idosos demonstraram que mulheres altamente treinadas mostraram uma melhoria na proliferação de células T induzidas por mitógeno em comparação com um grupo não treinado21. A melhoria da proliferação das células T também foi relatada noutro estudo de corredores idosos que treinaram uma média de 17 anos. Estes resultados foram associados com um melhor funcionamento do sistema imunitário adaptativo26 e sugerem que uma capacidade cardiovascular aumentada previne a acumulação de células T senescentes.
Devido a estas descobertas, Minuzzi et al.27 recrutaram 19 atletas master (mais de 40 anos) com 20 anos de experiência de treino e compararam o seu sistema imunitário com um grupo de controle sedentário composto por dez indivíduos com idades aproximadas. Neste estudo, os investigadores concluiram que o exercício tem a capacidade de não apenas prevenir a acumulação das células T senescentes ao longo da vida, como também de potenciar a sua exclusão através de mecanismos como a apoptose. Assim, estes dados revelam-nos que o treino físico regular é capaz de reverter as alterações associadas com a idade nas subpopulações de linfócitos e de reduzir parcialmente o declínio das funções das células T relacionadas com a idade.
Num estudo57 publicado recentemente (Março 2020), com dados recolhidos num hospital de Whuan (China), aparentemente a cidade que se tornou o epicentro da pandemia covid-19, os autores sugeriram que a linfopenia (contagem reduzida de linfócitos no sangue) é um indicador eficaz para predizer a severidade dos sintomas do covid-19 e propuseram um modelo de classificação de risco com base na percentagem de linfócitos no sangue. Neste trabalho, os autores verificaram que os indíviduos com uma percentagem de linfócitos mais baixa, tinham pior prognóstico e maior risco de mortalidade.
O músculo esquelético como um órgão imuno-regulador
O músculo esquelético é reconhecido como um órgão endócrino capaz de expressar e secretar citocinas (conhecidas como miocinas ou mioquinas) no sistema circulatório durante a actividade física28. A interleucina-6 (IL-6) foi a primeira miocina identificada e pode ser considerada uma das mais eficazes na regulação do sistema imunitário. A IL-6 é produzida logo após o início da actividade física e os níveis produzidos dependem de vários factores como a intensidade do exercício, a duração do exercício e a quantidade de massa muscular utilizada29. Na verdade, as nossas células musculares já produzem IL-6 basal mas o exercício pode aumentar essa libertação em mais de 100 vezes30.. Mas há aqui uma questão muito importante a destacar e que normalmente gera alguma confusão. Por um lado, a IL-6 produzida através das contracções musculares exerce um potente efeito anti-inflamatório (via c-Jun terminal kinase/activador proteína-131) que leva à produção de outros mediadores regulatórios como interleucina-10 (IL-10), receptor antagonista da interleucina-1 (IL-1RA) e à inibição do factor de necrose tumoral alfa (TNF-α) pelos monócitos e macrófagos32,33. Mais, a IL-6 também estimula a libertação de cortisol pelas glândulas supra-renais, proporcionando assim um segundo sinal anti-inflamatório34. Por outro lado, a IL-6 derivada da via de sinalização factor nuclear-kB (NF-kB35) tem um efeito pró-inflamatório e está naturalmente associada a estados de inflamação crónica e de fraca saúde. Recentemente, numa análise a 150 pacientes infectados de dois hospitais em Whuan (China), Ruan et. al.58, verificaram que as concentrações de IL-6 diferiam significativamente entre sobreviventes e não sobreviventes do covid-19, com os não sobreviventes a registar valores 1,7 vezes mais altos, indicando que a IL-6 elevada (não aquela derivada das contracções musculares) também tem repercussões negativas na imunidade. Pode fazer algumas respirações diafragmáticas agora 🙂
Além da IL-6, outras citocinas como a interleucina-736 (IL-7) e interleucina-1537 (IL-15), expressam-se também através das contracções musculares. A IL-7 é necessária para o desenvolvimento de timócitos38 e tanto a IL-7 como a IL-15 são factores proliferativos de linfócitos (especialmente para as células T ingénuas39), que têm tendência a diminuir com a idade e com a inactividade física40. A IL-15 proveniente do músculo ainda aumenta a actvidade das células natural killer (NK) e tem uma influência na redução de gordura através da inibição da lipogénese41. Outras miocinas libertadas pelos músculos também têm sido apontadas na literatura pelos seus efeitos metabólicos e imunológicos, contudo é importante ter presente que os músculos podem segregar mais de 600 miocinas e que ainda há muito por investigar nesta área de estudo, a que alguns autores já designam de “miocinoma”42.
De facto, o treino ao longo da vida também parece afectar os níveis basais de citocinas pró e anti-inflamatórias. Neste estudo levado a cabo por Minuzzi et. al.43, que teve como objectivo analisar os efeitos do envelhecimento e do treino ao longo da vida nas principais citocinas pró e anti-inflamatórias, ficou expresso que os níveis de IL-1RA, interleucina-1 beta (IL-1β), interleucina-4 (IL-4) e interleucina-8 (IL-8) de atletas master estavam mais equilibrados quando comparados com dois grupos sedentários de idade semelhante e de idade mais jovem.
Portanto, o músculo esquelético deve ser visto como a nossa farmácia endógena, um património importante a preservar ao longo da vida que vai ajudar a aumentar a imunidade. Uma reserva de nutrientes e aminoácidos que vai defender o corpo em situações de doença e na recuperação de qualquer evento traumático. Logo, um investimento no desenvolvimento de saúde e imunidade passa desde logo por manter a massa muscular e um estilo de vida activo.
Efeitos agudos e efeitos crónicos do exercício na imunidade
A evidência indica que os mecanismos associados à alteração da função imunitária com o exercício estão relacionados com vários factores, como estímulos do sistema neuroendócrino (catecolaminas, cortisol), estímulos metabólicos (i.e., hidratos de carbono, antioxidantes ou prostaglandinas)44,45, bem como com o débito cardíaco, fluxo sanguíneo, pressão arterial, forças de cisalhamento, entre outros. Alguns estudos parecem sugerir que os efeitos agudos do exercício (e.g., apoptose de algumas células) podem estimular a mobilização de células estaminais hematopoiéticas da medula óssea e de células imunes senescentes dos tecidos periféricos para a circulação46.
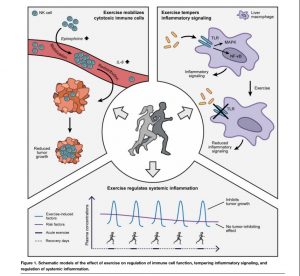
Mas a resposta imunitária aguda ao exercício depende da duração e intensidade do mesmo. No âmbito da revisão efectuada por Nieman et. al.4, os autores diferenciaram exercício moderado e vigoroso, utilizando um limiar de intensidade de 60% do VO2 máximo e frequência cardíaca de reserva, e um limiar de duração de 60 minutos. O exercício agudo estimula o intercâmbio de células e componentes do sistema imunitário inato entre os tecidos linfóides e o sangue. Embora transitório, ocorre um efeito cumulativo ao longo do tempo, com melhor vigilância imunitária contra agentes patogénicos, células cancerígenas e uma diminuição da inflamação sistémica4. É por este motivo que tanto a saúde como a imunidade constroem-se todos os dias e não com shots de imunidade, com exercício pouco consistente ou com programas de transformação corporal de curto prazo.
Durante exercícios aeróbios de intensidade moderada e vigorosa em períodos de duração inferior a 60 minutos, a actividade protectora dos macrófagos teciduais ocorre paralelamente a uma recirculação aprimorada de imunoglobulinas, citocinas anti-inflamatórias, neutrófilos, células NK, células T citotóxicas e células B imaturas, que são essenciais na melhoria da saúde imunitária e na saúde metabólica. Estas sessões curtas de exercício de intensidade moderada mobilizam preferencialmente as células NK e as células T CD8+, que exibem alta citotoxicidade e vão atacar especificamente as células infectadas. Ao longo do tempo esta imunovigilância vai aumentando e, naturalmente, o potencial terapêutico do exercício também.
Muitos estudos sustentam que altas cargas de trabalho, competições e o stress fisiológico, metabólico e psicológico associados estão ligados à disfunção imunitária, à inflamação, ao stress oxidativo e ao dano muscular. De facto, vários biomarcadores da função imunitária podem ficar alterados durante várias horas a dias durante a fase de recuperação, mas isto acontece especialmente no caso dos indivíduos que fazem exercício prolongado e intenso, como por exemplo maratonas. A ligação entre exercício intenso e prolongado e o aumento do risco de doença já tem sido estudada desde os anos 80 / início dos anos 90. Os primeiros estudos epidemiológicos indicaram que os atletas envolvidos em eventos de maratona, ultramaratona e/ou de intensidades muito elevadas estavam em risco aumentado de infecções do trato respiratório superior.
Na realidade, quando analisamos os estudos realizados neste âmbito (relação entre exercício vigoroso e doença), verificamos que a maioria foram realizados com atletas de endurance (maratonistas, ultramaratonistas, triatletas, nadadores, esquiadores) e com atletas de elite, indivíduos que são submetidos a cargas de trabalho e a níveis de stress bastante diferentes de um atleta recreativo. O custo de se tornar um atleta de elite será sempre a saúde e como tal não podemos comparar laranjas com maçãs. Embora Campbell et. al.47 tenham desafiado o significado clínico e a ligação entre esforço intenso e disfunção imunitária transiente (uma questão que irá ser explorada mais abaixo), a maioria dos investigadores na área da imunologia do exercício apoia a posição que o sistema imunitário reflecte a magnitude do stress fisiológico imposto ao seu praticante. Mas atenção, isto não significa que a intensidade não possa ser elevada, isto significa é que a intensidade e outras variáveis do treino precisam de ser geridas de forma criteriosa.
Influências clínicas do exercício crónico nas infecções respiratórias
Cada período de actividade física moderada promove melhorias transientes na imunovigilância e, quando repetida regularmente, confere múltiplos benefícios à saúde, incluindo menor incidência de doenças respiratórias e inflamação. Os ensaios clínicos randomizados (8 semanas a 1 ano de duração)21,49-53 são consistentes na demonstração que os indivíduos que participam em programas de exercício moderado ou meditação52,53, experimentam menor incidência e duração de infecções do trato respiratório superior. A magnitude da redução destes sintomas com a realização de exercícios moderados quase diários é geralmente de 40% a 50%, excedendo os níveis relatados para a maioria dos medicamentos e suplementos.
Neste estudo efectuado por Nieman et. al.48, foram seguidos durante 12 semanas um grupo de 1002 adultos (18-85 anos; 60% mulheres e 40% homens), metade durante o inverno e a outra metade durante o outono, com a finalidade de monitorizar os sintomas de infecções do trato respiratório superior. Os resultados indicaram que o número de dias com infecções respiratórias foi 43% menor em indivíduos envolvidos numa média de cinco ou mais dias por semana de exercício aeróbio (20 minutos ou mais) em comparação com os indivíduos sedentários (≤ 1 dia / semana) e 46% menor para aqueles que estavam em melhor forma física.
Adicionalmente, conforme referido na secção “efeitos do exercício na imunosenescência”, há também uma melhoria na resposta de anticorpos à imunização contra o vírus da gripe em idosos que incorrem em programas regulares de exercício físico20.
O mito da supressão imunitária induzida pelo exercício
Num artigo de revisão publicado há cerca de dois anos atrás, Campbell et. al47, colocaram algumas questões relevantes, que devem merecer a nossa atenção. Os estudos que indicaram um maior número de infecções do trato respiratório superior decorrentes da “actividade física”, além de terem sido auto-reportadas (i.e., não foram efectivamente medidas através de análises laboratoriais), foram realizados em maratonistas e ultramaratonistas, sugerindo que essas infecções têm maior probabilidade de acontecer quando a duração e a intensidade do exercício são muito elevadas. Por outro lado, é preciso ter presente que essas infecções poderão também ser o resultado de muitas outras causas, algumas mais directamente associadas com essas práticas desportivas (cargas de trabalho muito elevadas, alergia, asma, inflamação não específica das mucosas, hiperventilação própria do exercício, exposição a temperaturas mais frias) e outras de carácter mais geral mas não menos importantes (maior stress psicológico, ansiedade, deficiências nutricionais, exposição a grandes aglomerados populacionais, fadiga, sono inadequado, viagens e adaptação a novos fusos horários, desidratação). Isto significa que o sistema imunitário poderá já estar em maior risco antes de iniciar o exercício. Assim, da mesma forma que existe evidência (com as devidas limitações) a confirmar que o exercício pode aumentar o risco de infecção, também existem vários estudos epidemiológicos a indicar que o exercício pode reduzir o risco de infecção, inclusivamente em atletas de elite, que estão sujeitos a elevadas cargas de trabalho.
Outro pilar da imunologia do exercício que recebeu considerável atenção nas últimas três décadas é a avaliação das alterações induzidas pelo exercício na imunidade das mucosas, principalmente através da medição dos níveis de anticorpos da imunoglobulina A (IgA) na saliva. A função principal da IgA é prevenir a entrada de organismos invasores na circulação e como tal a sua concentração aumentada ou diminuída poderá revelar uma imunidade mais forte ou mais fraca, respectivamente. Mais uma vez, os estudos aqui estão divididos e os autores apontam várias limitações que podem deturpar a secrecção de IgA: os níveis absolutos de IgA relatados não controlaram adequadamente a quantidade de saliva produzida; o estado da saúde oral é raramente avaliado; ritmo circadiano; stress psicológico; género; etnia, doença; medicamentos; tabaco e fase do ciclo menstrual. Pelo que é arriscado dizer-se que quaisquer alterações subtis na IgA salivar após o exercício reflectem a supressão imunitária e um risco aumentado de infecções oportunistas.
Já constatamos que o sistema imunitário é estimulado durante o exercício mas nas horas após o exercício, geralmente é observado que a frequência e capacidade funcional dos linfócitos do sangue periférico diminui para níveis inferiores ao pré-exercício, levando alguns autores a propor que o exercício induz uma janela de imunosupressão, fenómeno designado de “janela aberta”. Mas em vez de suprimir a competência imune, um ponto de vista mais actual é que essa linfopenia aguda e transitória 1 a 2h após o exercício é benéfica para a vigilância e regulação imunitária. De facto, no que parece ser uma resposta altamente especializada e sistemática, tem sido proposto que o exercício vai, por via da estimulação adrenérgica e libertação de adrenalina, mobilizar as células imunitárias para a circulação e depois redistribuir essas mesmas células para os tecidos periféricos (i.e., superfícies mucosas como pulmões, intestino, pele) para conduzir a vigilância imunológica e providenciar feedback à medula óssea para iniciar a produção de novas células imunitárias. Estas células imunitárias são recrutadas do baço, dos nódulos linfáticos, do intestino e de células imobilizadas ao longo das paredes vasculares. Esta redistribuição das células imunitárias (em particular das células NK) é, na verdade, um dos mecanismos apontados para a redução dos tumores em pacientes com cancro54,55 (infelizmente esta forma de imunoterapia ainda não é levada a sério) e o seu aumento é proporcional à intensidade do exercício56.
Para haver adaptações significativas ao nível do treino é preciso que o mesmo seja progressivamente intenso. Intenso não significa necessariamente mais longo, significa intenso para o indivíduo que está a realizar o exercício. E para fazê-lo de forma responsável, é preciso atender ao seu historial clínico, à sua mobilidade articular e à sua capacidade de trabalho, ou seja, é preciso avaliar o indivíduo para poder compreender a sua tolerância. Um indivíduo que treina de forma consistente há muitos anos terá respostas diferentes ao nível do sistema imunitário quando comparado com um indivíduo sedentário ou pouco regular no exercício. Tal como qualquer intervenção cirúrgica, o exercício também precisa de ser bem administrado para ser eficaz.
Conclusão
Vivemos numa cultura de elevado sedentarismo em que não é necessário fazer qualquer tipo de esforço físico para sobreviver. As pessoas habituaram-se a não fazer nada do ponto de vista físico para sobreviver mas agora de repente parece que descobriram que podem e devem ser mais activas. A disseminação de exercícios sem critério e de aulas online gratuitas nestes últimos tempos tem sido própria da histeria que se vive num arraial. A falta de consciência de alguns profissionais, que certamente estão a tentar ajudar, também não tem ajudado. O que mais me preocupa nesta história toda é que na internet vale tudo e não há qualquer tipo de filtro. E devido a esta falta de cultura e literacia física colectiva, a maior parte das pessoas não tem educação suficiente para distinguir o bom do mau, nem o excelente do medíocre. Qualquer coisa serve, independentemente se tem qualidade ou não.
Para quem não sabe para onde vai qualquer caminho serve, disse o gato na célebre história de Alice no País das Maravilhas, em resposta à sua exclamação “eu não sei para onde quero ir!”. Esta questão do covid-19 veio confirmar que a atitude diária das pessoas rege-se mais pelo medo, que pelos seus objectivos e desejos. Os media sabem disso e exploram muito bem essa fragilidade das pessoas. O bombardeamento de informação sobre esta matéria tem sido estridente e hoje em dia é cada vez mais difícil distinguir a verdade da mera opinião de jornalistas e de pseudo-especialistas. O medo é o principal supressor do sistema imunitário, o cortisol e as hormonas do stress vão superar a energia necessária para combater a infecção. Esta é uma questão que decorre da nossa evolução enquanto espécie, se estivesse doente e tivesse que fugir de um animal que me queria fazer mal, eu iria canalizar toda a minha energia para esse efeito, ou seja, eu iria lutar com todas as minhas forças para combater esse animal. A situação do covid-19 veio confirmar também que temos uma população débil que investe muito pouco no desenvolvimento da sua saúde e imunidade. E quanto maior o número de comorbilidades, sinais e sintomas de perda de saúde, maior é o risco de adoecer e morrer.
Em relação ao exercício físico, e com base na revisão de literatura efectuada e na nossa experiência prática no acompanhamento de indivíduos imunossuprimidos, maioritariamente doentes oncológicos, há várias coisas que deve fazer para aumentar a sua imunidade e bem-estar geral. Aqui ficam as principais recomendações:
- Mantenha-se o mais activo possível e evite passar muito tempo seguido sentado. Passar muito tempo sentado é altamente nocivo! Tenha presente que o movimento sempre foi uma necessidade essencial à vida humana e afecta todos os sistemas e órgãos do corpo. O facto de hoje não ter problemas de saúde devido ao seu comportamento sedentário é apenas uma questão de tempo. (nota: manter-se activo no seu dia a dia não é igual a manter as suas articulações, a sua postura, a sua musculatura e a sua competência de movimento em bom estado. Para optimizar a sua função corporal e retirar maiores benefícios precisa de dedicar tempo à avaliação e ao tratamento da sua condição músculo-esquelética).
- Seja consistente na sua adesão ao exercício físico. Procure formas de exercício prazerosas, que lhe permita manter uma frequência semanal elevada (5-6x por semana, idealmente). A intensidade deverá naturalmente oscilar entre moderada e vigorosa. Há um efeito cumulativo na construção da imunidade. Os indivíduos que são mais consistentes ao nível da sua prática de exercício estruturado têm menor incidência de doenças, registam uma maior eficácia ao nível da vacinação e têm um sistema imunitário mais vigilante. A prática de meditação também tem mostrado resultados na prevenção de infecções respiratórias, e é importante na gestão do stress e na melhoria do bem-estar geral.
- Em função da sua condição, privilegie formas de exercício seguras que permitam realizar intensidades elevadas de curta duração (a evidência aponta como limiar 60 minutos de duração) ao invés de intensidades elevadas de longa duração. A lógica do “no pain, no gain” é simplesmente imbecil e só faz sentido se você não estiver preocupado com a sua saúde e longevidade. Os eventos de endurance de intensidade elevada poderão suprimir o sistema imunitário e aumentar o risco de doença e infecção do trato respiratório, especialmente se não tiver os cuidados adicionais na sua preparação. No que diz respeito à intensidade, podemos compreendê-la de duas formas: 1) intensidade ao nível da activação neuromuscular / contracção muscular (com a utilização de vários protocolos de treino de força) e 2) intensidade ao nível da capacidade dos sistemas energéticos (com a utilização de vários protocolos de treino de métodos intervalados e/ou de métodos contínuos). Intensidades elevadas, se pensarmos numa escala de 1 a 10, em que 1 é pouco intenso e 10 muito intenso, referimo-nos a uma percepção de esforço de oito para cima.
- Em função da sua condição, privilegie programas de treino baseados no desenvolvimento de motricidade e literacia física, que fomentem a (re)aprendizagem de padrões de movimento fundamentais (agachar, empurrar, puxar, levantar, carregar, rodar, locomoção) de forma assistida ou resistida, com variabilidade de movimento consequente, no desenvolvimento atlético e que envolvam maiores quantidades de massa muscular. Quanto maior a massa muscular envolvida e a intensidade aplicada, maior será a comunicação cruzada entre os seus músculos e os vários sistemas do corpo, entre os quais o sistema imunitário. Reforço mais uma vez: a intensidade pode ser benéfica mas precisa de ser bem gerida. Não esqueçamos aquela célebre frase utilizada na Medicina: a dose certa é o que diferencia o veneno do remédio.
- Em função da sua condição, privilegie programas de treino que potenciem o desenvolvimento de mobilidade articular, de força e de massa muscular. O desenvolvimento de mobilidade vai melhorar a saúde das suas articulações, optimizar amplitudes de movimento e desbloquear o seu potencial de movimento. O desenvolvimento de força será fundamental para manter a autonomia motora e a independência funcional nas tarefas diárias / desportivas. O desenvolvimento de massa muscular irá contribuir para aumentar a sinalização anti-inflamatória e imuno-reguladora ao longo da sua vida. O músculo é a farmácia endógena do ser humano mas este precisa do estímulo certo para poder manter-se saudável e funcional.
Finalmente, se ainda está a pensar nos 60 minutos de duração do exercício como o critério fundamental para a sua prática, não está a pensar bem. O aspecto mais importante será mesmo a prescrição de exercício com qualidade, será a qualidade do exercício que irá resolver os seus problemas de saúde, melhorar a sua função corporal e o seu bem-estar geral. Porque se o mesmo for prescrito com qualidade a duração da sua prática torna-se um factor acessório.
Bons treinos!
Pedro Correia
Referências:
1. Weyh C, Krüger K, Strasser B. Physical Activity and Diet Shape the Immune System during Aging. Nutrients. 2020 Feb 28;12(3). pii: E622. doi:10.3390/nu12030622. Review. PubMed PMID: 32121049.
2. Van Dijk JG, Matson KD. Ecological immunology through the lens of exercise immunology: new perspective on the links between physical activity and immune function and disease susceptibility in wild animals. Integr Comp Biol 2016;56:290–303.
3. Larrabee RC. Leukocytosis after violent exercise. J Med Res (NS) 1902;7:76–82.
4. Nieman DC, Wentz LM. The compelling link between physical activity and the body’s defense system. J Sport Health Sci. 2019 May;8(3):201-217. doi:10.1016/j.jshs.2018.09.009. Epub 2018 Nov 16. Review. PubMed PMID: 31193280;PubMed Central PMCID: PMC6523821.
5. Janeway C. Immunobiology: The Immune System in Health and Disease. London, UK: Current Biology Publications (1999).
6. Reed RG, Raison CL. Stress and the immune system. In: E Charlotte editor. Environmental Influences on the Immune System. Vienna: Springer (2016). 97–126. doi: 10.1007/978-3-7091-1890-0_5.
7. AwD, Silva AB, Palmer DB. The effect of age on the phenotype and function of developing thymocytes. J Comp Pathol. (2010) 142 Suppl 1:S45–59. doi: 10.1016/j.jcpa.2009.10.004.
8. Palmer DB. The effect of age on thymic function. Front Immunol. (2013) 4:316. doi: 10.3389/fimmu.2013.0031.
9. Agrawal A, Agrawal S, Gupta S. Dendritic cells in human aging. Exp Gerontol. (2007) 42:421–6. doi: 10.1016/j.exger.2006.11.007.
10. Agrawal A, Agrawal S, Tay J, Gupta S. Biology of dendritic cells in aging. J Clin Immunol. (2008) 28:14–20. doi: 10.1007/s10875-007-9127-6.
11. Montecino-Rodriguez E, Berent-Maoz B, Dorshkind K. Causes, consequences, and reversal of immune system aging. J Clin Invest. (2013) 123:958–65. doi: 10.1172/JCI64096.
12. Akunuru S, Geiger H. Aging, clonality, and rejuvenation of hematopoietic stem cells. Trends Mol Med. (2016) 22:701–12. doi: 10.1016/j.molmed.2016.06.003.
13. Michaud M, Balardy L, Moulis G, Gaudin C, Peyrot C, Vellas B, et al. Proinflammatory cytokines, aging, and age-related diseases. J Am Med Dir Assoc. (2013) 14:877–82. doi: 10.1016/j.jamda.2013.05.009.
14. Mosser DM, Edwards JP. Exploring the full spectrum of macrophage activation. Nat Rev Immunol. (2008) 8:958–69. doi: 10.1038/nri2448.
15. Watad A, Bragazzi NL, Adawi M, Amital H, Toubi E, Porat BS, et al. Autoimmunity in the elderly: insights from basic science and clinics – a mini-review. Gerontology (2017) 63:515–23. doi: 10.1159/000478012.
16. Ramos-Casals M, García-Carrasco M, Brito MP, López-Soto A, Font J. Autoimmunity and geriatrics: clinical significance of autoimmune manifestations in the elderly. Lupus (2003) 12:341–55. doi: 10.1191/0961203303lu383ed.
17. Simpson, R.J.; Lowder, T.W.; Spielmann, G.; Bigley, A.B.; LaVoy, E.C.; Kunz, H. Exercise and the aging immune system. Aging Res. Rev. 2012, 11, 404–420.
18. Duggal, N.A.; Niemiro, G.; Harridge, S.D.R.; Simpson, R.J.; Lord, J.M. Can physical activity ameliorate immunosenescence and thereby reduce age-related multi-morbidity? Nat. Rev. Immunol. 2019, 19, 563–572.
19. A. R. Pascoe, M. A. Fiatarone Singh, and K. M. Edwards, “The effects of exercise on vaccination responses: a review of chronic and acute exercise interventions in humans,” Brain, Behavior, and Immunity, vol. 39, pp. 33–41, 2014.
20. A. L. de Araújo, L. C. Silva, J. R. Fernandes et al., “Elderly men with moderate and intense training lifestyle present sustained higher antibody responses to influenza vaccine,” Age (Dordrecht, Netherlands), vol. 37, no. 6, p. 105, 2015.
21. Nieman, D.C.; Henson, D.A.; Gusewitch, G.; Warren, B.J.; Dotson, R.C.; Butterworth, D.E.; Nehlsen-Cannarella, S.L. Physical activity and immune function in elderly women. Med. Sci. Sports Exerc. 1993, 25, 823–831.
22. Bartlett, D.B.; Fox, O.; McNulty, C.L.; Greenwood, H.L.; Murphy, L.; Sapey, E.; Goodman, M.; Crabtree, N.; Thøgersen-Ntoumani, C.; Fisher, J.P.; et al. Habitual physical activity is associated with the maintenance of neutrophil migratory dynamics in healthy older adults. Brain Behav. Immun. 2016, 56, 12–20.
23. Frydelund‐Larsen, L., Penkowa, M., Akerstrom, T., Zankari, A., Nielsen, S. and Pedersen, B.K. (2007), Exercise induces interleukin‐8 receptor (CXCR2) expression in human skeletal muscle. Experimental Physiology, 92: 233-240.
24. Timmerman, K. L., Flynn, M. G., Coen, P. M., Markofski, M. M. & Pence, B. D. Exercise training- induced lowering of inflammatory (CD14+CD16+) monocytes: a role in the anti- inflammatory influence of exercise? J. Leukoc. Biol. 84, 1271–1278 (2008).
25. Bartlett, D. B. et al. Ten weeks of high- intensity interval walk training is associated with reduced disease activity and improved innate immune function in older adults with rheumatoid arthritis: a pilot study. Arthritis Res. Ther. 20, 127 (2018).
26. Shinkai, S.; Kohno, H.; Kimura, K.; Komura, T.; Asai, H.; Inai, R.; Oka, K.; Kurokawa, Y.; Shephard, R.J. Physical activity and immune senescence in men. Med. Sci. Sports Exerc. 1995, 11, 1516–1526.
27. Minuzzi, L.G.; Rama, L.; Chupel, M.U.; Rosado, F.; Valente dos Santos, J.; Simpson, R.J.; Martinho, A.; Paiva, A.; Teixeira, A.M. Effects of lifelong training on senescence and mobilization of T lymphocytes in response to acute exercise. Exerc. Immunol. Rev. 2018, 24, 72–84.
28. Pedersen, B. K. & Febbraio, M. A. Muscles, exercise and obesity: skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 8, 457–465 (2012).
29. Pedersen BK, Steensberg A, Keller P, et al. Muscle-derived interleukin-6: lipolytic, anti-inflammatory and immune regulatory effects. Pflügers Arch Eur J Physiol. 2003;446(1):9-16. doi:10.1007/s00424-002-0981-z.
30. Pedersen BK, Febbraio MA. Muscle as an Endocrine Organ: Focus on Muscle-Derived Interleukin-6. Physiol Rev. 2008;88(4):1379-1406. doi:10.1152/physrev.90100.2007.
31. Whitham, M. et al. Contraction-induced interleukin-6 gene transcription in skeletal muscle is regulated by c-Jun terminal kinase/activator protein-1. J. Biol. Chem. 287, 10771–10779 (2012).
32. Munoz- Canoves, P., Scheele, C., Pedersen, B. K. & Serrano, A. L. Interleukin-6 myokine signaling in skeletal muscle: a double- edged sword? FEBS J. 280, 4131–4148 (2013).
33. Starkie, R.; Ostrowski, S.R.; Jauffred, S.; Febbraio, M.; Pedersen, B.K. Exercise and IL-6 infusion inhibit endotoxin-induced TNF-alpha production in humans. FASEB J. 2003, 17, 884–886.
34. Bethin, K. E., Vogt, S. K. & Muglia, L. J. Interleukin-6 is an essential, corticotropin- releasing hormone- independent stimulator of the adrenal axis during immune system activation. Proc. Natl Acad. Sci. USA 97, 9317–9322 (2000).
35. Liu, T., Zhang, L., Joo, D. et al. NF-κB signaling in inflammation. Sig Transduct Target Ther 2, 17023 (2017).
36. Haugen, F. et al. IL-7 is expressed and secreted by human skeletal muscle cells. Am. J. Physiol. Cell Physiol. 298, C807–C816 (2010).
37. Rinnov, A. et al. Endurance training enhances skeletal muscle interleukin-15 in human male subjects. Endocrine 45, 271–278 (2014).
38. Shitara, S. et al. IL-7 produced by thymic epithelial cells plays a major role in the development of thymocytes and TCRγδ+ intraepithelial lymphocytes. J. Immunol. 190, 6173–6179 (2013).
39. Wallace, D. L. et al. Prolonged exposure of naive CD8+ T cells to interleukin-7 or interleukin-15 stimulates proliferation without differentiation or loss of telomere length. Immunology 119, 243–253 (2006).
40. Duggal, N. A., Pollock, R. D., Lazarus, N. R., Harridge, S. & Lord, J. M. Major features of immunesenescence, including reduced thymic output, are ameliorated by high levels of physical activity in adulthood. Aging Cell 17, 12750 (2018).
41. Duggal, N.A., Niemiro, G., Harridge, S.D.R. et al. Can physical activity ameliorate immunosenescence and thereby reduce age-related multi-morbidity?. Nat Rev Immunol 19, 563–572 (2019).
42. Whitham M, Febbraio MA. The ever-expanding myokinome: Discovery challenges and therapeutic implications. Nat Rev Drug Discov 15(10): 719-729, 2016.
43. Minuzzi, L.G.; Chupel, M.U.; Rama, L.; Rosado, F.; Muñoz, V.R.; Gaspar, R.C.; Kuga, G.K.; Furtado, G.E.; Pauli, J.R.; Teixeira, A.M. Lifelong exercise practice and immunosenescence: Master athletes cytokine response to acute exercise. Cytokine 2019, 115, 1–7.
44. Mazdarani FH, Khaledi N, Hedayati M. Effects of official basketball competition on the levels of cortisol and salivary immunoglobulin (A) among female children. J Childhood Obesity (2016) 1:12.
45. Pedersen BK, Toft AD. Effects of exercise on lymphocytes and cytokines. Br J Sports Med. (2000) 34:246–51. doi: 10.1136/bjsm.34.4.246.
46. Cao Dinh H, Beyer I, Mets T, Onyema OO, Njemini R, Renmans W, et al. Effects of physical exercise on markers of cellular immunosenescence: a systematic review. Calcif Tissue Int. (2017) 100:193–215.
47. Campbell JP, Turner JE. Debunking the myth of exercise-induced immune suppression: redefining the impact of exercise on immunological health across the lifespan. Front Immunol 2018;9:648.
48. Nieman DC, Henson DA, Austin MD, Sha W. Upper respiratory tract infection is reduced in physically fit and active adults. Br J Sports Med 2011;45:987–92.
49. Nieman DC, Nehlsen-Cannarella SL, Markoff PA, Balk-Lamberton AJ, Yang H, Chritton DB, et al. The effects of moderate exercise training on natural killer cells and acute upper respiratory tract infections. Int J Sports Med 1990;11:467–73.
50. Nieman DC, Nehlsen-Cannarella SL, Henson DA, Koch AJ, Butterworth DE, Fagoaga OR, et al. Immune response to exercise training and/or energy restriction in obese women. Med Sci Sports Exerc 1998;30:679–86.
51. Chubak J, McTiernan A, Sorensen B, Wener MH, Yasui Y, Velasquez M, et al. Moderate-intensity exercise reduces the incidence of colds among postmenopausal women. Am JMed 2006;119:937–42.
52. Barrett B, Hayney MS, Muller D, Rakel D, Ward A, Obasi CN, et al. Meditation or exercise for preventing acute respiratory infection: a randomized controlled trial. Ann Fam Med 2012;10:337–46.
53. Barrett B, Hayney MS, Muller D, Rakel D, Brown R, Zgierska AE, et al. Meditation or exercise for preventing acute respiratory infection (MEPARI-2): a randomized controlled trial. PLoS One 2018;13: e0197778. doi:10.1371/journal.pone.0197778.
54. Christensen JF, Simonsen C, Hojman P. Exercise Training in Cancer Control and Treatment. Compr Physiol. 2018 Dec 13;9(1):165-205.
55. Hojman P. Exercise protects from cancer through regulation of immune function and inflammation. Biochem Soc Trans. 2017 Aug 15;45(4):905-11. doi:10.1042/BST20160466. Epub 2017 Jul 3. Review. PubMed PMID: 28673937.
56. Campbell JP, Riddell NE, Burns VE, Turner M, van Zanten JJ, Drayson MT, Bosch JA. Acute exercise mobilises CD8+ T lymphocytes exhibiting an effector-memory phenotype. Brain Behav Immun. 2009 Aug;23(6):767-75.
57. Tan, L., Wang, Q., Zhang, D. et al. Lymphopenia predicts disease severity of COVID-19: a descriptive and predictive study. Sig Transduct Target Ther 5, 33 (2020).
58. Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020 Mar 3. doi: 10.1007/s00134-020-05991-x. [Epub ahead of print] Erratum in: Intensive Care Med. 2020 Apr 6;:.PubMed PMID: 32125452; PubMed Central PMCID: PMC7080116.
Dado os tempos que vivemos, em que o contacto social está condicionado, proliferam a promoção de serviços à distância em todas as áreas profissionais. Na área do fitness, parece que se descobriu de repente que se pode (e deve) treinar todos os dias e que se pode treinar em casa ou sozinho. É incrível a explosão de publicações nas redes sociais por parte de personal trainers a oferecerem alinhamentos de exercícios para as pessoas executarem em casa. Sabemos que, para uma melhor saúde e resiliência, é fundamental que se faça exercício físico todos os dias, tal como é fundamental alimentar-se e manter a higiene pessoal, mas isto sempre foi assim e, portanto, não é uma necessidade apenas dos tempos actuais. Por isso, publicar um alinhamento de exercícios para todos fazerem vale tanto quanto publicar uma foto do prato de comida ou a lavar os dentes. Serve quanto muito para lembrar-lhe que essas actividades são importantes, mas o conteúdo não é, em grande medida, aplicável a si que lê este texto. Muito menos no que concerne ao exercício. Aliás, pegar no garfo e faca para comer, ou o acto de lavar os dentes são actividades menos complexas do que a execução da maior parte dos exercícios físicos que vemos frequentemente propostos e muito menos a sua organização numa sessão de treino.
A saúde e resiliência resultante do treino é ainda mais relevante em tempos de crise como os que estamos a viver, mas foi sobretudo construída nos meses e anos prévios a este momento. Nomeadamente durante os tais meses e anos que você foi consistentemente ao ginásio fazer o seu treino, muitas vezes com sacrifício. Custa organizar-se de forma a conseguir treinar! Temos família e trabalho e por vezes é complicado conciliar todas as obrigações sociais e profissionais com horários destinados à nossa saúde e bem-estar, neste caso ao treino. E reparem que agora sim falo de treino.
Porque muitos de vocês que estão a ler estas linhas perceberam há muito a diferença entre “fazer exercícios” e treino. Perceberam que “fazer exercícios” é melhor que nada, mas que o treino está a um nível acima. O treino é um processo e obriga a organizar todas as suas variáveis no tempo. Obriga a fazer uma avaliação cuidada da condição inicial, seleccionar exercícios e formas de execução específicas, a observar e avaliar movimento, e fazer os ajustes necessários (e.g. carga, tipo e forma de execução de exercícios) por forma a garantir constante progressão nessa senda da saúde, performance e resiliência. Treinar não é o mesmo que ‘’fazer exercícios” sempre variados e sem critério apenas com o intuito de manter alguma actividade física. E porque alguns percebem essa diferença, têm vindo ao longo dos meses e anos que antecederam os tempos de hoje a fazer os tais sacrifícios organizacionais. E optaram por investir um pouco mais do seu tempo e dinheiro, e regularmente deslocaram-se a um ginásio para obter um serviço de treino. Um serviço em que um programa é seguido, os exercícios não são escolhidos de forma aleatória, e em que a progressão nas cargas utilizadas bem como a execução dos exercícios é monitorizada de perto por um treinador.
Todos os benefícios do treino personalizado são possíveis obter à distância via online. Considero que a forma presencial será sempre superior, mas mediante boa organização e compromisso do treinador e aluno é possível uma progressão constante e essa diferença ser mitigada. Como é que na The Strength Clinic sabemos isso? Porque já o fazemos há vários anos! Além disso, o treino personalizado online pode até ter algumas vantagens em relação ao treino presencial, tais como:
- Não ter que se deslocar ao ginásio a determinada hora. Este aspecto pode ser uma grande vantagem para algumas pessoas. Se for garantida a auto-disciplina de cumprir o seu programa de treino, o tempo de deslocação e o que isso implica em termos organizacionais é poupado. Além disso, poderá escolher uma hora de treino que melhor encaixe no seu horário sem estar condicionado pela disponibilidade do seu treinador;
- Maior consistência e empenho na execução dos exercícios. Visto que pode escolher a hora do seu treino, corre menos riscos de falhar a sua sessão de treino pois terá mais flexibilidade em adaptar o horário. Dessa forma, garante mais facilmente a frequência semanal de treinos desejável. Além disso, como recomendamos que documente em vídeo um resumo de cada treino numa plataforma online para que o seu treinador possa observar, isso encerra também um compromisso adicional no cumprimento da sessão e na boa execução dos exercícios;
- Melhor custo benefício. De facto, poderá usufruir de quase todos os benefícios dum treinador pessoal por um valor mais baixo porque não terá que pagar pelo valor relacionado com despesas de funcionamento e material do local onde ocorreria a sessão de treino presencial;
- Treinar directamente com o seu treinador preferido. Se o treinador com quem gostaria de trabalhar não tem disponibilidade presencial ou o seu valor presencial é acima das suas possibilidades, a alternativa online irá possibilitar trabalhar directamente com ele.
A mensagem “não deixe de treinar mesmo que seja em casa ou sozinho” no contexto das adversidades que vivemos hoje está correcta! Contudo, esta necessidade não surgiu hoje. É algo que deveria fazer parte das nossas vidas se nos queremos manter mais fortes e saudáveis desde sempre. Para este efeito, treinar é muito melhor do que apenas “fazer exercícios”, sobretudo se retirados de publicações nas redes sociais sem qualquer critério ou consciência corporal e sem programação futura. Serve apenas para “mexer o corpo” e ficar cansado no momento, mas não passará disso mesmo. Porque treinar implica um processo que tem por base os seus objectivos e características individuais. Numa sessão de treino, aquilo que se faz hoje foi em função do que se fez ontem e do que se vai fazer no futuro. E é possível continuar a treinar online e retirar todos os benefícios do treino personalizado, mesmo que à distância. Obriga a um empenho mútuo do aluno e treinador num processo que é conjunto. Esse desenvolvimento pessoal optimizado será sempre o nosso compromisso na The Strength Clinic para consigo. Estamos aqui para guiá-lo nesse processo e não para oferecer treinos “chapa 5” para todos!
Bons treinos!
Nuno Correia

The International Society of Sports Nutrition published in 2017 a position stand (see reference below) on the safety and efficacy of creatine supplementation in the context of exercise, sports and medicine.
Creatine supplementation, one of the most popular and studied nutritional supplements, has in fact been shown to be effective in improving athletic performance (especially in high intensity exercise) and inducing relevant training adaptations. The consequent increase in intramuscular creatine (and phosphocreatine) reserves facilitates the rapid re-synthesis of ATP, the so-called energy “currency” of the body, which is essential for almost every reaction in our body. Thus, the increased availability of creatine in the cell through supplementation contributes to improve performance because it increases the energy availability in order to exercise (i.e. muscle contraction) as well as a whole range of other muscle cell related reactions. Creatine supplementation can in fact enhance strength production, muscle work, accelerate recovery and help preventing injury.
Additionally, creatine supplementation appears to be highly safe and effective not only in athletes but also in non-athletes (such as the so-called exercise enthusiasts), as well as in various clinical populations. In fact, several studies (see ISSN article, reference below) point to benefits of creatine supplementation in various populations and clinical settings, such as:
– Accelerating injury rehabilitation (because it attenuates muscle atrophy);
– Protection of neuronal injuries (spinal and cerebral);
– Mitigation of debilitating consequences in people with congenital syndromes of creatine synthesis deficiency;
– Attenuating the progression of neurodegenerative diseases (e.g. Huntington’s disease, disease, Parkinson’s disease, mitochondrial diseases, amyotrophic lateral sclerosis);
– Prevention and / or improvement of bioenergetics in patients with myocardial ischemia or stroke victims;
– Improving metabolic and functional indicators associated with aging;
– Possible benefit during pregnancy for optimal growth, development and health of the fetus.
In conclusion, creatine does indeed appear to be a safe and beneficial nutritional supplement for a wide range of populations and ages. Indeed, this is a supplement that actually works!
Take creatine and power to you!
Nuno Correia
References:
Kreider, R.B. et al., 2017. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14(1), p.18. Available at: http://jissn.biomedcentral.com/articles/10.1186/s12970-017-0173-z.
A International Society of Sports Nutrition (ISSN) publicou um “position stand” em 2017 (ver referência abaixo) acerca da segurança e eficácia da suplementação com creatina no contexto do exercício, desporto e medicina.
A suplementação com creatina, um dos mais populares e estudados suplementos nutricionais, tem de facto mostrado ser eficaz em melhorar a performance atlética (sobretudo em exercício de alta intensidade) e induzir adaptações ao treino relevantes. O aumento consequente das reservas intramusculares de creatina (e fosfocreatina) facilita a ressíntese rápida de ATP, denominada como “moeda de troca” energética essencial para quase todas as reacções no nosso corpo. Assim, o aumento da disponibilidade de creatina na célula através da suplementação contribui para melhorar o desempenho, pois aumenta a disponibilidade de energia para exercício (i.e., contracção muscular), bem como para todo um espectro de outras reacções relacionadas com as células musculares. De facto, suplementação de creatina pode aumentar a capacidades de produção de força, trabalho muscular, acelerar a recuperação e ajudar a prevenir lesões.
Adicionalmente, a suplementação com creatina parece ser altamente segura e eficaz não só em atletas mas também em não-atletas (tais como os chamados entusiastas do exercício físico) e ainda em várias populações clínicas. De facto, vários estudos (ver artigo da ISSN, referência abaixo) apontam para benefícios na suplementação de creatina nas mais variadas populações e contextos clínicos, tais como:
– Acelerar a reabilitação de lesões (porque atenua a atrofia muscular);
– Protecção de lesões neuronais (medulares e cerebrais);
– Atenuar as consequências debilitantes em pessoas com síndromas congénitos de deficiência de síntese de creatina;
– Atenuar a progressão de doenças neurodegenerativas (e.g. doença de Huntington, doença de Parkinson, doenças mitocondriais, esclerose lateral amiotrófica)
– Prevenir e/ou melhorar a bioenergética em pacientes com isquemia do miocárdio ou vítimas de acidente vascular cerebral;
– Melhorar indicadores metabólicos e funcionais associados ao envelhecimento;
– Possível benefício durante a gravidez para o óptimo crescimento, desenvolvimento e saúde do feto.
Em conclusão, a creatina parece de facto ser um suplemento nutricional seguro e com benefícios para as mais variadas populações e idades. Este é um suplemento que de facto funciona!
Desfruta do poder da creatina!
Nuno Correia
Referências:
Kreider, R.B. et al., 2017. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14(1), p.18. Available at: http://jissn.biomedcentral.com/articles/10.1186/s12970-017-0173-z.

In order to maintain physical function, recover better from injury, maintain lean mass and stay healthier overall, older individuals need a higher protein intake than younger individuals. Higher protein intake contributes for attenuating inflammatory and catabolic processes, as well as ameliorating the decreased efficiency in protein metabolism associated with age.
According to the recommendations advanced by the PROT-AGE Study Group (2013) (reference below), older individuals should:
– eat at least 1 to 1.2g/kg body weight of protein per day;
– eat MORE protein if suffering from acute or chronic illness, between 1.2-1.5g/kg body weight of protein per day;
– ingest EVEN MORE if malnourished and / or suffering from severe illness or injury, ~2g/kg body weight of protein per day;
– limit protein intake if suffering from SEVERE KIDNEY DISEASE and NOT following hemodialysis. These individuals are therefore an EXCEPTION concerning protein intake;
– use supplementation to the achieve desired protein intake levels;
– and, of course, DO the type of exercise that most effectively promotes the maintenance or increases in lean mass, which is strength training.
And no, kidney disease is NOT caused by protein intake. In a one-year follow-up study with resistance-trained men consuming ~2.51-3.32 g/kg of body weight per day for one year, there were no harmful effects on measures of blood lipids as well as liver and kidney function (Antonio et al, 2016).
Maintaining strength and lean mass (including muscle mass, bone and connective tissue mass) are identified as the first and most relevant biomarkers of health and longevity. Improving these markers produces a positive and powerful “domino effect” on most (probably all) of the other health markers. Proper protein intake and strength training is essential for building lean mass. And even more crucial as we age in order to counteract the inevitable progressive loss of efficiency in our metabolism.
Do not fear protein nor strength training. These are probably two of your best allies to live better and longer.
Don’t forget the protein at your next meal!
Nuno Correia
References:
Bauer, J. et al., 2013. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the prot-age study group. Journal of the American Medical Directors Association, 14(8), pp.542–559.
Antonio, J., Ellerbroek, A., Silver, T., Vargas, L., Tamayo, A., Buehn, R., & Peacock, C. A. (2016). A High Protein Diet Has No Harmful Effects: A One-Year Crossover Study in Resistance-Trained Males. Journal of nutrition and metabolism, 2016, 9104792.

In previous articles (check Part 1 and Part 2) we discussed the fact that while all golfers will do everything possible to change their game (buying new clubs and new balls), many overlook one of the most decisive factors for their physical and mental success – their nutrition; we have identified some of the main reasons why golfers never change and, finally, we have pointed out five important links between golf and proper nutrition. In this article, I will share with you my concerns about the so called “normal diet” and the five most important habits you should create to start nourishing your body better.
The Western Diet
The western diet is generally used to describe popular eating habits in the USA. As these eating habits are still very popular in Europe and other parts of the non-Western world, it will probably be necessary to find a new name for this type of “diet” in the coming years (perhaps the killer diet is a good name!).
But what is the “western diet?” Well, this “diet” can be briefly characterized by a high intake of processed foods, refined carbohydrates, sugar and hydrogenated fats; and a low intake of healthy fruits, vegetables and fats. It is this “western diet” that has been associated with most western diseases or diseases of civilization (examples: cardiovascular disease, obesity, diabetes, cancer, Alzheimer, Parkinson). Interestingly, this diet may also be responsible for increased violence and decreased cognitive test scores in school-age children (attention deficit disorder) and adults. Finally, this “western diet” has also been linked to bone loss (osteoporosis) and muscle wasting (sarcopenia) in adult individuals.
Let’s look at an example of a “normal athlete” daily menu before working with me.
Breakfast: Bowl of cereals and milk + Natural orange juice + Coffee with sugar
Snack 1: Mixed toast + Chocolate milk
Lunch: Chicken salad with mayonnaise and ketchup sauce + soda + ice cream
Snack 2: Slice of cake + Juice
Dinner: Grilled fish with vegetables + Baked potatoes + Glass of red wine + Dessert
For most people, this may even be considered a good day (and indeed there are some good things in this menu), but in the long run this type of eating will greatly compromise your health and performance. For this reason, we have to discuss this situation with the person and meet their real physiological and functional needs.
The Habits you must create
Before changing their diet, it is important that people start with a firm and solid foundation, and then make the necessary changes to optimize their health and performance. Most people (athletes included) want to start building a house from the roof down or building walls without paying attention to the quality of the soil. Any of these habits are simple enough, but just like any habit you want to create, it takes time to practice to assimilate the foundations of proper nutrition.
Habit 1 – Drink more water
Sometimes we talk about so much about food and forget about water, the most important element our bodies need to function properly. It is water that regulates all the functions of our body, including the activity of all solutes (the solid materials) dissolved in it. It is water that will actually allow the nutrients we consume to reach our cells and our organs. Aim to consume 1-2 glasses of water after waking up and to drink about 2 liters / day.
Habit 2 – Eat a protein source at every meal
Eating protein at every meal is critical. Of course, some “experts” will make you believe otherwise, suggesting that protein is somehow harmful to the kidneys, unnecessary, etc. However, I want to highlight the fact that what I am looking for my clients / athletes is the best of these three worlds: better health, better body and better performance – it will be very difficult to achieve these three with a suboptimal protein intake. Some examples include: eggs, meat, fish, chicken, turkey and shellfish.
Habit 3 – Eat vegetables at every meal
Your parents and / or grandparents are right – you need to eat vegetables to prevent disease! Evidence has shown that in addition to the micronutrients (vitamins and minerals) contained in vegetables, there are also phytochemicals that are essential for optimal physiological functioning. Vegetables will help improve the acid-base balance in the body, so my advice is eating all the vegetables you can!
Habit 4 – Eat a healthy fat sources at every meal
Fat (such as protein) is an essential macronutrient and so we have to ensure proper intake every day through our diet. There has been a lot of misconception about the effects of fat on diet but the truth is that fat can be our best friend when the goal is to lose fat mass, optimize the body’s physiological response and our health. Some examples of healthy fats include: fatty fish, nuts, seeds, extra virgin olive oil, coconut and avocado.
Habit 5 – Eat more vegetables with main meals and leave the other carbohydrates to the post workout window
Another way of saying this is: if you have fat to lose, you have to earn the right to eat carbohydrates by doing vigorous exercise in the first place! Do you want to keep eating bread, pasta, rice, potatoes, crackers, sugary foods, pizzas, sweets, etc.? You can even eat them – just make sure you do it in the post workout window (1-2 hours after training) because this is the time when your body is most sensitive to insulin. As for the quality of carbohydrates, you will have more benefits if you choose gluten-free foods (rice, quinoa, chestnuts, sweet potatoes, yams, potatoes) than highly processed foods or gluten-free junk foods. Also, don’t use exercise as an excuse to treat your body like the garbage truck!
Good strokes!
Pedro Correia

Ever wonder why most people eat so much alike? Milk and cereals for breakfast, a soup and a sandwich at lunchtime, and, with luck, a slightly more balanced dinner of meat or fish, rice and some vegetables? What about those mid-morning and/or afternoon coffee and toast snacks? Crackers? Cakes and sodas? Cereal bars? Do you think this is a coincidence? Of course not, this is no coincidence!
This only happens this way because that is how you were taught to eat. Maybe this is the way your parents eat. Perhaps this is the way your wife, husband or partner eats. Maybe this is the way your friends and/or co-workers eat. Maybe this is the way your teammates eat. In fact, people do not even realize if what they are eating is appropriate or not for our physiology and genetics, if it improves or worsens health, if it improves or worsens performance, they eat this way because this is the eating pattern that they have been following for many years, and these were the habits they have ingrained.
In the last article we covered several reasons why golfers neglect nutrition, one of the aspects that can most influence their performance on the golf course. Interestingly, most golfers are more concerned with top-of-the-range clubs and new accessories than the foods they eat. And that is why today I will present five reasons for you to improve your diet.
Think about this for a while. If you knew that eating and/or supplementing in a certain way would: 1) reduce your fat mass; 2) increase your muscle strength; 3) improve your bone health; 4) enable a faster recovery; 5) increase your distance from the tee; 6) improve your mood; 7) reduce feelings of anxiety and anger; 8) improve your concentration and creativity; 9) improve virtually any known health marker and 10) improve your performance in training sessions and/or competition, would you be willing to eat that way? Given this short list of benefits I think it would be worth a try. Stay with me.
- Eating well will improve your body composition
Your total body weight is the sum of your lean mass and your fat mass. Lean mass consists of muscle mass, organs, bones, blood and skin. Your fat mass is basically all the fat that has accumulated in the body. For an individual to be considered athletic, he or she needs to maintain a good ratio between lean mass and fat mass. And golfers should be no exception. By this I do not mean that all golfers need to have Cristiano Ronaldo’s abs, what I mean is that under normal circumstances excess body fat has no benefits (unless you are a sumo wrestler in the spare time). Excess body fat will affect the efficiency of your swing, your mobility and your rotational power, meaning that you will have greater difficulty moving your body when you carry excess fat. The more fat you have, the more energy you have to use to move your body – the fat will “steal” power from your swing. So, it’s not the fat tissue that will give you power, it’s your muscle tissue!
- Eating well will improve recovery
If you are seriously committed to improving your game, you know you need to practice (and a lot!). According to experts, some professional golfers can hit 600 balls a day including chips and putts. And to perform all these swings you need muscle strength and power, meaning you need to do some kind of work in the gym! If the body is not prepared to cope with this type of stress in a regular basis, injuries and pain will begin to rise. If you often end your golf training sessions sore, if you notice fluctuations in motivation, if you can no longer hit balls in a coordinated manner, if you notice reductions in appetite, and if you are awake at night despite training a lot, it is very likely that your recovery is not being optimized. Muscle damage, Central Nervous System fatigue, and over-reaching are all common symptoms of many sports, but golfers tend to ignore these things. Although golf is not as physically demanding as other sports, the fact is that the daily training volume to which the body is subjected is large and this will make nutrition a key part of recovery.
- Eating well will improve mood, concentration and focus
Any professional golfer on the PGA Tour and/or the European Tour is capable of winning any major event. But why do some stand out more consistently than others? Because, according to experts, those who excel are mentally unshakable. That is, their ability to turn off negative internal dialogue, to consciously relax the brain and to focus with unflappable concentration is impressive. Some consider this to be an innate skill. And it is indeed. But it can be trained! However, there is also a biochemical basis for this mental prowess. You should know that by providing the right nutrients, including nutritional supplements, at the right times, the physiological link between the brain and muscles can be strengthened. Such as focus and concentration. For example, by controlling your blood glucose levels with frequent meals and less dietary sugar, mood fluctuations and that feeling of low energy after lunch can be eliminated. Therefore, in addition to body composition and recovery, nutrition can strongly affect your mental game. With the right nutrients, concentration, neuromuscular efficiency and mood can be significantly improved. On the contrary, if you do not ingest good nutrients, fatigue will appear earlier and you will no longer be able to concentrate in the same way.
- Eating well will improve your health
When I am talking about health, I am not just referring to the absence of pain and/or illness, I mean a feeling of physical, emotional and mental well-being. To perform at the highest level, health needs to be optimized, so the definition of health I share with my clients/athletes includes: 1) a resilient immune system; 2) strong antioxidant systems that protect against free radicals; 3) good detoxification systems; 4) a good balance of bacteria in the gut; 5) a good balance of basic and acid foods; 6) low levels of inflammation in the body; 7) an ideal balance between fat mass and lean mass; 8) a good balance of fatty acids; 9) good insulin sensitivity; 10) high energy levels and 11) the ability to maximize mental and physical performance at any age. All of these health markers can be influenced by the foods we eat every day! Therefore, these nutritional strategies will not only help you prevent disease but also optimize your body function and perform at the highest level.
- Eating well will improve your performance in training and competition
It is not surprising to most of you to find that most nutrition on the golf course is poor, ranging from mixed sandwiches and beer, to sports drinks and “energy bars” (note: most of which are basically full of sugar and bad fats) with a seemingly healthy label. These foods are certainly not preparing you for noteworthy performances, I would even say that these foods will compromise your performance. For example, beer is a central nervous system depressant, reducing concentration and motor control. Sports drinks (e.g. Powerade), sandwiches (even wholegrain!) and “energy bars” will raise blood sugar levels, which is-apparently good because it leads to a quick energy rise, but it turns out to be bad because then we’ll also watch a rapid energy drop 45-60 minutes later. When blood sugar levels drop to a peak, mood worsens, focus and concentration decrease – and of course performance worsens!
To optimize your performance in training and competition, there are at least three things that are required. First, you must maintain good hydration, especially in hot and humid climates. Even a slight dehydration can reduce coordination and motor control. Secondly, you must control your blood sugar levels. This means that you should not eat sugar-rich foods, but foods that help keep your blood glucose levels stable. Third, you should resort to some nutritional strategies and/or supplements that help you increase focus and concentration. In short, don’t continue to depend on what they offer you in the golf course bar carts – probably the only healthy thing they have there is water!
Good strokes!
Pedro Correia

All golfers have one thing in common: they will invest a lot of time and money to improve their game! They will hire the best coaches to perfect your golf swing. They will buy the best equipment available to get more accuracy and to gain distance. Those who have already realized the importance of fitness in this sport will hire the best professionals to help them gain mobility, become stronger and more resilient. Some will turn to sports psychologists to learn how to maintain a good attitude in the field, focus and concentration. They do all this in order to make more birdies. But aren’t they forgetting something?
In fact, there is something that most golfers forget to change: their low-quality diet. Most golfers have no idea how diet can influence performance. For starters, they forget that eating poorly will compromise increased muscle strength and will lead to body fat accumulation. And if you still think that having weak muscles and excess body fat is the way to go to become a top-level golfer, it’s not worth reading any further. This article is not for you.
In addition to the deleterious effects on body composition and muscle strength it must be borne in mind that eating poorly will limit focus and concentration, will lead to mood swings and may lead to poor immune function, increased chronic inflammation and general health problems. Try playing several rounds for days at a time when you are in a bad mood, in bad shape, and unable to concentrate. Poor nutrition will have a direct impact on training and competition. Lack of focus, concentration and early tiredness, especially during training and / or competitions, are signs that your nutrition is compromising your performance.
No doubt, you can be very skillful with your golf clubs, do some Ballesteros shots and do some exceptional rounds from time to time, but if you’re looking for consistency in results and longevity as a golfer, there’s no better substitute than the foods you eat every day. None!
So why do golfers never change?
There are several reasons why golfers never change and prefer to continue eating the club sandwiches, the chips and the pasta served in every clubhouse menu in the world. Let’s go through some of those reasons.
1) The myth of the pre-competition meal.
Many golfers (especially beginners) make the mistake of thinking that it is only the food eaten before and during practice and competition that can affect their game. While this may make sense at a first glance, this is not physiologically what happens – most of the energy you are using today depends on the nutrients you have eaten (and absorbed) in the last 72 hours!
Please note, I am not saying that what you eat before and after practice / competition makes no difference. Of course it does! However, these meals are not necessarily the most important. Each meal will have a certain impact on your body regardless of the time frame in which it is consumed. It is the cumulative effect of these meals that will lead to an improvement (or decrease) in performance.
In other words, in golf, there is no pre-competition or intra-competition magic meal. If you’ve waited until the day before a big competition to start eating well, it’s probably too late. I am sorry to inform you but there are no miraculous solutions, you really need to eat consistently well!
2) Golfers cannot see the link between nutrition and performance.
Most golfers do not realize the connection between nutrition and performance. And that’s because they are not aware of how diet will influence their muscle function and brain biochemistry.
In the case of golf, as this is a sport that does not involve too much energy expenditure and does not require athletes to maintain a certain body weight (as with wrestlers, gymnasts, swimmers, endurance athletes or athletes from other sports), it is thought that the need to eat well is not that important. In fact, this relationship might not seem so obvious.
But that’s not the point, golfers don’t need to be muscular and low body fat individuals as you see in fitness magazines. What they need is to develop their athletic potential so that this is not a factor that could hinder their performance on the golf course. Golf is not a very energy-intensive sport so a golfer’s nutritional needs cannot match those of a fighter or an endurance athlete. But different does not mean less important – as we saw above it is not just body composition that will be influenced by diet.
Although the link between golf and nutrition is a little less visible than in other sports, it exists. Maintaining and / or increasing muscle mass, mobility, reducing inflammation of muscles and joints, maintaining focus and concentration, preventing injuries, can all be influenced by nutrition. But only those who put the best nutritional strategies into practice will have competitive advantages (obviously this does not include Big Macs!).
3) The difficulty in changing eating habits.
Probably the most difficult hurdle for most people is overcoming the eating habits they have. Our eating patterns have been around for a long time and few people are willing to change them if there is not a strong reason (as in the case of a serious health problem). And why does this happen? Because we have not been taught to think that food is information for our cells. We have not been taught to think that food will influence the expression of our genes. We have not been taught to think that it is the everyday foods we consume from our environment that can trigger health improvement or health deterioration.
Of course there are many other reasons why golfers are reluctant to change their eating habits and why you don’t change yours. And that’s why in the next article I will continue to address this topic so you can understand why you need to change your eating habits quickly to live healthier and to take your game to the next level.
Good strokes!
Pedro Correia

“People don’t decide their future, people decide their habits and their habits decide their future.”
– F.M. Alexander
Nine years ago (2010)1, the European Working Group on Sarcopenia in Older People (EWGSOP) published a definition of sarcopenia that has been widely used worldwide and this definition has fostered advances in the identification and care of people at risk or with sarcopenia. It was defined as a syndrome characterized by progressive and widespread loss of muscle mass and strength at risk of adverse outcomes such as physical disability, poor quality of life and death. Because the relationship between muscle mass and strength is not linear (the ability to generate strength is not only dependent of muscle mass), the criteria for its diagnosis included low muscle mass and low muscle function (i.e. strength or physical performance).
After learning that in 2016 sarcopenia was classified as a disease by the World Health Organization, as noted in the first part of this article, the EWGSOP22 updated its operational definition and various diagnostic strategies, considering now that muscle strength (measured by grip strength or the chair stand test) is the main parameter for measuring muscle function, even more important than the amount of muscle mass. Therefore, it is in this context that we justify the title of this article and reinforce the importance of sharing this message with all health professionals.
The implications of this condition on human health are several and widely known: increased risk of falls and fractures3,4; impairment of activities of daily living5; association with heart disease6; respiratory disease7 and cognitive dysfunction8; lower quality of life9; loss of independence10,11,12 and death13. In financial terms, public health costs have also been calculated in several papers. In a study by Janssen et. al.14, in 2004, the costs of sarcopenia in the United States were estimated at $ 18.5 billion annually, representing about 1.5% of total health costs. In a study conducted here in Portugal at the Hospital de Santo António in Porto and published in 201615, it was found that hospitalization costs associated with sarcopenia were higher by 58.5% for patients under 65 years and by 34% for patients aged 65 and over. More recently (2018), the Hertfordshire Cohort Study in the United Kingdom16 found that the costs associated with lack of muscle strength were estimated at £ 2.5 billion annually.
In the present scenario, where the phenotype of unhealthy aging is proliferating in the eyes of all industrialized nations, in which diseases such as hypertension, cancer, depression, Alzheimer’s disease and type II diabetes are destroying people’s lives, it is essential to adopt measures aimed at improving function of each individual rather than diagnosing illnesses and administering medicines which, in addition, do not help solving this problem, and may further aggravate their condition. We know that the main health problems are related to poor diet, physical inactivity, lack of sleep, excess alcohol, exposure to tobacco and polluted environments but also lack of movement quality, vigor and muscular strength.
The benefits of strength training in health are well supported in the scientific literature and the most important ones are: decrease in blood pressure; decreased risk of osteoporosis and sarcopenia; improvement of lipid profile; increased cardiorespiratory capacity; prevention and management of chronic pain; increased insulin sensitivity; improvement of wellbeing and self-confidence. Moreover, several studies17,18,19 have shown a strong and consistent correlation between increased strength and muscle mass with decreased mortality, reinforcing the fact that the decline in strength associated with the current levels of sedentarism and aging need to be addressed. Therefore, a well-designed strength training program that meets the individual’s competency and follows the principles of adaptation to training will improve all of the above health indicators and all the necessary physical qualities (strength, power, speed, agility, balance, coordination, mobility, endurance) to carry out the activities of our daily life. These are the parameters of physical function that are currently being proposed as biomarkers of aging in humans20.
Consequently, program design will be the determining factor in this equation. And while it is true that this process requires imperative knowledge of sports sciences, it must be borne in mind that it also requires field work and art in coaching. Instead of being so preoccupied with following the guidelines and looking for statistically significant results, we should be concerned that our approach is relevant to one’s life. Because we work with people. People who have time constraints to train. People with different family and professional responsibilities. People who have different lives from each other. People who have a host of metabolic and / or orthopedic problems that no randomized controlled trial can ever reproduce! Yes, this is a complex process.
Finally, we know that one of the mechanisms responsible for muscle atrophy, sarcopenia and aging is apoptosis, a form of programmed cell death and a fundamental process in aging. But when we train, eat and rest properly, we are sending a signal to our body to create an anabolic environment, an environment that enhances the release of growth factors and suppresses apoptosis. That is, strength training is a macroscopic growth factor that suppresses programmed cell death (i.e. apoptosis), but unlike drugs, where an increasing in dose means more disease and dependence, an increase in load (even if reduced) means more health, more strength and more vigor. This way, the daily decisions will always be up to each one: treat the body like a Ferrari or treat the body like a rental car.
Pedro Correia
References:
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing 2010; 39: 412–23.
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jan 1;48(1):16-31.
- Bischoff-Ferrari HA, Orav JE, Kanis JA et al. Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos Int 2015; 26:2793–802.
- Schaap LA, van Schoor NM, Lips P et al. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: the longitudinal aging study Amsterdam. J Gerontol A Biol Sci Med Sci 2018; 73: 1199–204.
- Malmstrom TK, Miller DK, Simonsick EM et al. SARC-F: a symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J Cachexia Sarcopenia Muscle 2016; 7: 28–36.
- Bahat G, Ilhan B. Sarcopenia and the cardiometabolic syndrome: a narrative review. Eur Geriatr Med 2016; 6: 220–23.
- Bone AE, Hepgul N, Kon S et al. Sarcopenia and frailty in chronic respiratory disease. Chron Respir Dis 2017; 14: 85–99.
- Chang KV, Hsu TH, Wu WT et al. Association between sarcopenia and cognitive impairment: a systematic review and metaanalysis. J Am Med Dir Assoc 2016; 17: 1164.e7–64.e15.
- Beaudart C, Biver E, Reginster JY et al. Validation of the SarQoL(R), a specific health-related quality of life questionnaire for Sarcopenia. J Cachexia Sarcopenia Muscle 2017; 8: 238–44.
- Dos Santos L, Cyrino ES, Antunes M et al. Sarcopenia and physical independence in older adults: the independent and synergic role of muscle mass and muscle function. J Cachexia Sarcopenia Muscle 2017; 8: 245–50.
- Akune T, Muraki S, Oka H et al. Incidence of certified need of care in the long-term care insurance system and its risk factors in the elderly of Japanese population-based cohorts: the ROAD study. Geriatr Gerontol Int 2014; 14: 695–701.
- Steffl M, Bohannon RW, Sontakova L et al. Relationship between sarcopenia and physical activity in older people: a systematic review and meta-analysis. Clin Interv Aging 2017; 12: 835–45.
- De Buyser SL, Petrovic M, Taes YE et al. Validation of the FNIH sarcopenia criteria and SOF frailty index as predictors of long-term mortality in ambulatory older men. Age Ageing 2016; 45: 602–8.
- Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R. The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc. 2004 Jan;52(1):80-5.
- Sousa AS, Guerra RS, Fonseca I, Pichel F, Ferreira S, Amaral TF. Financial impact of sarcopenia on hospitalization costs. Eur J Clin Nutr. 2016 Sep;70(9):1046-51. doi: 10.1038/ejcn.2016.73. Epub 2016 May 11.
- Pinedo Villanueva, R. A., Westbury, L. D., Syddall, H. E., Sanchez, M., Dennison, E. M., Robinson, S. M., & Cooper, C. (2018). Health care costs associated with muscle weakness: a UK population-based estimate. Calcified Tissue International.
- Ruiz JR, Sui X, Lobelo F, et al. Association between muscular strength and mortality in men: prospective cohort study. BMJ. 2008;337(7661):a439. Published. doi:10.1136/bmj.a439.
- Srikanthan P, Karlamangla AS. Muscle mass index as a predictor of longevity in older adults. Am J Med. 2014;127(6):547-53.
- Dos Santos L, Cyrino ES, Antunes M, Santos DA, Sardinha LB. Changes in phase angle and body composition induced by resistance training in older women. Eur J Clin Nutr. 2016 Dec;70(12):1408-1413. doi: 10.1038/ejcn.2016.124. Epub 2016 Jul 13. PubMed PMID: 27406159.
- Cadore EL, Izquierdo M. Muscle Power Training: A Hallmark for Muscle Function Retaining in Frail Clinical Setting. J Am Med Dir Assoc. 2018 Mar;19(3):190-192.

There is currently sufficient scientific evidence to assert that strength training is an effective method for preventing, treating and potentially reversing various chronic diseases. Indeed, adherence to a properly designed strength training program can significantly increase the physical and mental health of the population.
The importance is such that several world-renowned organizations (World Health Organization, Centers for Disease Control and Prevention, American Heart Association, American Association for Cardiovascular and Pulmonary Rehabilitation, American College of Sports Medicine) recommend this form of training for maintain health.
However, despite this evidence, most of exercise recommendations are still for aerobic training, and few physicians (and health professionals in general) recommend strength training. This article aims to alert for the relevance and valuable impact of strength training on health.
About 100% of our biological existence has been dominated by outdoor activity. Hunting and searching for food has been a condition of human life for millions of years1. That is, if in the past it took effort (i.e. physical activity) to find food, nowadays food comes to us without having to make any effort. Therefore, we have moved from a very active lifestyle to a highly sedentary lifestyle. With serious consequences for public health. If in the past all people had to engage in some sort of physical exertion to carry out their daily tasks, today most of them do not have those needs. The environment has changed and so have people. They are weaker, sicker, have more chronic pain and are increasingly dependent on medicines. But the message still going on in our society (and passed on in medical appointments) is “make no physical efforts and follow your normal life”. And I believe this is the worst advice people can get! Normal life? But what kind of advice is this? How can normal be good? You must be completely alienated from reality in order to make such recommendations.
Today we have more opportunities than ever to build a healthy and strong phenotype. The phenotype is the expression of our organism, and it depends largely on the choices we make every day. Two organisms can have the same genotype, the same DNA, but different phenotypes – based on their experiences and the environment. Admittedly, there are things we cannot control such as our genetic heritage, the place of the world where we were born / lived, overall luck and the general environment to some extent. But there are many things that we can control that depend solely on our priorities in life and our daily choices (examples: exercise habits, eating, sleeping, stress management, smoking, alcohol, exposure to polluted environments). And I believe that exercise in general (and strength training in particular) is the most important factor of all. It is the most potent, it’s quantifiable and acts quickly on all systems and organs of the human body.
The reality is this: the population is aging and with more chronic / noncommunicable diseases. The main noncommunicable diseases are cardiovascular diseases, cancers, chronic respiratory diseases and diabetes. These four disease groups alone account for over 80% of the 41 million deaths in the world2! According to the first report on healthy aging by the World Health Organization (WHO), the number of people over 60 is expected to double by 20503, and it is in this context that we need to urgently intervene to promote motor autonomy and improve people’s functional capacity. Traditional recommendations for walking, swimming, Pilates, and “doing low effort activities” or “no physical effort” probably need to be reconsidered and properly contextualized.
It is in this context that strength training and athletic training play a key role. All people (athletes and non-athletes) need to train their physical qualities to live with quality and independently. After age 30, adults lose 3-8% of their muscle mass per decade. Over time, the loss of lean mass contributes to a decrease in muscle strength and power, which are important predictors of balance, falls and mortality4. In the case of the elderly, it is important to note that falls are the main cause of accidental death after age 65 and hip fractures are those that most affect their independence5.
When I speak of strength I mean the basis for interacting with the environment around us, the foundation for the development of other physical qualities (mobility, power, speed, agility, muscle endurance), the ability to produce strength against external resistance (it can be the floor or any other object) through muscle contractions. This is probably the most trainable capacity we have and the one that could have the greatest impact on improving our function, independence and functional longevity. Tasks such as brisk walking, sitting and rising from a chair, climbing stairs, maintaining balance, carrying luggage, or playing with children / grandchildren are examples of activities in our daily lives that require a minimal component of various manifestations of strength (maximum strength, power and strength endurance). Therefore, both strength and muscle (quality rather than quantity) are physical function related parameters that need to be taken care of in the quest for achieving a healthy aging phenotype.
These issues are even more important when we note that as of 1st of October 2016, in the tenth revision of the International Classification of Diseases (ICD-10), sarcopenia has been classified as a disease by WHO and has its own code (M62.84). This should lead to increased availability of diagnostic tools and increased enthusiasm for the pharmaceutical industry to develop drugs to combat sarcopenia6. But in my opinion, this also represents a great opportunity for exercise professionals to be able to help fighting this disease, as strength training (properly oriented of course) will be the most potent stimulus in its prevention and treatment.
Pedro Correia
References:
- Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Comprehensive Physiology. 2012;2(2):1143-1211. doi:10.1002/cphy.c110025.
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet, 2016; 388(10053):1659-1724.
- Beard JR, Officer A, de Carvalho IA, et al. The world report on ageing and health: A policy framework for healthy ageing. Lancet 2016;387:2145e2154.
- English KL, Paddon-Jones D. Protecting muscle mass and function in older adults during bed rest. Current Opinion in Clinical Nutrition and Metabolic Care. 2010;13(1):34-39. doi:10.1097/MCO.0b013e328333aa66.
- National Center for Injury Prevention and Control of the Centers for Disease Control and Prevention. Preventing Falls: A Guide to Implementing Effective Community-Based Fall Prevention Programs 2nd edition. Atlanta: 2015.
- Anker SD, Morley JE, von Haehling S. Welcome to the ICD-10 code for sarcopenia. J Cachexia Sarcopenia Muscle. 2016 Dec;7(5):512-514. Epub 2016 Oct 17. PubMed PMID: 27891296; PubMed Central PMCID: PMC5114626.

We often hear reports from people who spend hours and hours in the gym and remain the same. They do not lose fat, do not gain lean mass, do not gain strength, nor improve their functional capacity. They simply do not evolve. We also have those who rely only on the traditional weight training component to lose weight and yet not always have results, regardless of the diet they follow.
So, what is the secret for having results? Program design and professional supervision may be more important than you think.
In a study conducted by Bea et al. (2010), the authors investigated the association of exercise frequency and volume (total weight lifted on the military press and squat exercises) with changes in body composition in postmenopausal women who participated in a progressive strength training program for six years.
The women were divided into three groups: one group did strength training during this period, one started strength training after one year and the third (control group) did nothing. The training programs were supervised by professionals and involved motivational strategies to increase adherence. The training program consisted of eight exercises (based on free weights and machines) and was done three times a week, progressively.
The results showed that the group that did nothing (control group) gained weight and fat over the six years, suggesting something that everyone should already know: if nothing is done, we will get fatter and weaker with each passing day.
But there is something more interesting to highlight. The authors analyzed the relationship between body fat and increased squat load and found that the women who gained the most strength had better control of their weight and body composition over time! This means that if you are always doing the same program without managing training variables and principles, stagnation is what will happen.
So, what we have to tell you is that if you are part of that package that spends hours in the gym, between exercise machines, selfies and talking to your partner, then you are certainly not on your way to good results. We know that the socialization part is important and should not be ignored, we simply believe that it must be well managed! The key is knowing how to clearly distinguish what is training and what is ‘’going to the gym’’. And more training time is merely a quantitative indicator, not a quality indicator.
Enjoy your training!
Pedro Correia
References:
Bea JW, Cussler EC, Going SB, Blew RM, Metcalfe LL, Lohman TG. Resistance Training Predicts Six-Year Body Composition Change in Postmenopausal Women. Medicine and science in sports and exercise. 2010;42(7):1286-1295. doi:10.1249/MSS.0b013e3181ca8115.

Check Part 1 HERE and Part 2 HERE
Implications and practical applications of calorie restriction and intermittent fasting
And now … can the practice of calorie restriction (CR) or fasting have therapeutic value in humans? As noted earlier (Part 1), randomized controlled trials in humans studying the effects of CR and fasting in humans are scarcer. It is not easy to find volunteers to subject themselves to the “discomfort” of eating less food.
Just an aside …
Changing something in someone’s diet can be a daunting task! In fact, and based on my experience, people are generally highly resistant to changing whatever their eating patterns are and tend to defend them tooth and nail! They elaborate the most varied rationales (and very sophisticated sometimes … like the typical “but my grandfather is 90 years old and always ate this and that”) to justify the intake of certain foods that, essentially, they are just used to or like eating. Nutrition is like a religion for some, believe me …!
Back to human studies …
The other practical reason for the lack of controlled randomized human trials on the effects of CR or fasting to study its effects on life expectancy and the incidence of “age-related diseases” is that human life expectancy is long. However, some randomized controlled trials in humans point to clear benefits of CR practice in certain populations. Listed below are some of these studies, type of intervention and significant effects observed.
• Wang et al. (2013)
- Sample: obese individuals.
- Intervention: 5 days of 30% CR (low-fat / high-carb or high-fat / low-carb) after isocaloric diet period.
- Significant results:
- CR diets decreased fasting insulin and leptin levels by increasing free fatty acid levels (indicating mobilization of fat stores);
- Insulin sensitivity did not improve significantly (perhaps due to the short 5-day period), however muscle insulin signaling (in response to insulin) increased only in the low-fat / high-carb diet subjects. Note that this effect on insulin signaling in response to the low-fat / high-carb diet (rather than the high-fat / low-carb diet) may represent only a transient adaptive response due to the higher glycemic load in the diet. The short duration of the study does not allow the conclusion of a sustained improvement in insulin regulation.
- Kitzman et al. (2016)
- Sample: elderly obese individuals (67 ± 5 years) with heart failure.
- Intervention: 20 weeks of CR (350-400kcal / day deficit) with or without exercise (1 hour walking 3 days per week).
- Significant results:
- Both CR and exercise (separately) increased aerobic capacity (indicated by increase in VO2 peak), with even greater effects if combined;
- Both CR and exercise (separately) improved body composition (fat loss) with even greater effects if combined;
- CR (but not exercise) reduced the inflammatory marker C-reactive protein (CRP) and correlated with weight loss.
- Snel et al. (2012)
- Sample: obese individuals with type 2 diabetes mellitus (T2DM) and insulin-dependent.
- Intervention: 16 weeks of CR (450kcal / day) with or without exercise (1 hour + 4 30-minute sessions on a cycle ergometer per week).
- Significant results:
- Both CR and exercise improved fasting glucose, insulin and glycosylated hemoglobin (HbA1c) levels;
- The RC + exercise group lost more fat and waist circumference compared to the CR group only;
- Both CR and exercise increased insulin receptor expression and signaling (revealed by muscle biopsy) as well as peripheral insulin sensitivity.
- Pedersen et al. (2015)
- Sample: overweight or obese, non-diabetic individuals with coronary artery disease.
- Intervention: 12 weeks of CR (800-1000kcal / day) with or without exercise (3 days / week interval aerobic sled).
- Significant results:
- Separately, CR was superior to exercise in weight loss, fat mass and waist circumference, as well as fasting blood glucose, insulin sensitivity and glucose tolerance. However, CR led to better results combined with the exercise program.
- Razny et al. (2015)
- Sample: non-diabetic obese individuals
Intervention: 3 months CR (1200-1500 kcal / day) with or without 1.8 g / day omega-3 fatty acids (in a 5: 1 DHA / EPA ratio).
- Significant results:
- CR with or without omega-3 supplementation resulted in similar decrease in body weight and fat mass;
- CR had a superior positive effect on triglyceride and insulin levels when combined with omega-3 supplementation;
- Sample: non-diabetic obese individuals
RC + omega-3 (but not only CR) improved indicators of insulin resistance (HOMA index).
- Prehn et al. (2016)
- Sample: postmenopausal obese women.
- Intervention: 12 weeks CR (<800kcal / day) followed by 4 weeks on an isocaloric diet or 16 weeks on an isocaloric diet (control group). Recommendation to increase physical activity per week.
- Significant results:
- CR (but not the isocaloric diet) resulted in better scores on memory performance tests;
CR (but not the isocaloric diet) resulted in improved glycemic control and HbA1c levels;
- CR-induced increase in cerebral gray matter density was negatively correlated with glucose levels.
- CR (but not the isocaloric diet) resulted in better scores on memory performance tests;
Recommendations and Conclusions
In fact, CR or fasting interventions do indeed appear to have clear therapeutic utility in improving health parameters related to obesity, inflammation, insulin resistance, oxidative stress, and cardiac function. It is important to note that just reducing the amount of food you eat may not be enough and perhaps not recommended. Such a simplistic and long-term intervention can result in nutritional deficits and thereby boycott putative positive health outcomes. It is therefore important to monitor and ensure adequate nutrient levels through supplementation and / or in choosing nutritionally dense foods. Also noteworthy are the positive synergistic effects that CR seems to have when combined with exercise (Snel et al., 2012; de Luis et al., 2015; Kitzman et al., 2016), which may be prescribed concomitantly. In this context, a very mild CR intervention (e.g. 10% deficit) or short intermittent fasting periods (> 14 hours and does not need to be daily) combined with exercise may have very positive effects and are likely to have higher compliance compered to more aggressive fasting or CR interventions.
Of course, severe and prolonged CR with no exercise (especially strength training) can induce lean mass loss that is highly undesirable if the goal is to improve health. Once again, and as with almost everything, the secret lies in the right dosage! In certain populations such as pregnant women (or women trying to conceive) and young growing individuals, prolonged CR interventions should be avoided as they may compromise development. However, I emphasize again that the most important thing is not to ingest “calories” but ingest “nutrients”! In older individuals with sarcopenia, CR should perhaps be avoided, although the most determining factors for reversing sarcopenia are strength training and adequate protein intake (which should be higher for older individuals (> 2g / kg bodyweight).
Regarding the specific case of intermittent fasting (note: the focus of this article is not to discuss the use of intermittent fasting as a fat loss and / or maintenance strategy or muscle mass gains in the sports context, but rather its potential for general health benefits) although few, the available randomized controlled trials in humans indicate that intermittent fasting do offer beneficial effects similar to those of constant CR and perhaps is easier to implement (Donati et al., 2008; Marzetti et al., 2009; Alirezaei et al., 2010; Arum et al.; 2014; Godar et al., 2015). Irregular fasting episodes (e.g. not eating breakfast once or twice a week on non-training days) can not only be a strategy easy to implement strategy as a mean to control total weekly calories ingested, and it also has positive hormonal effects is mediated by some of the mechanisms described above. “Hormesis” is defined as a mild stressor that is beneficial to health, stress resistance, growth and longevity. It results from exposure to an “adequate” dose of a stressor. CR or fasting (or exercise) is something that we are evolutionarily designed to tolerate, and which at the right dose gives us benefits and greater resilience. The occasional stress of not eating can be a “healthy discomfort”!
Until next time!
Nuno Correia

What mechanisms underlie the effects of calorie restriction or intermittent fasting on longevity and “age-related diseases”?
But after all what is “getting old” … and why …?
Aging has been characterized by several authors as a process of progressive deterioration of molecular, cellular and tissue structures and functions that is conditioned by genetic and environmental factors (Hu & Liu, 2014). This multifactorial and complex process resulting from this progressive loss of function makes the individual more vulnerable to disease and ultimately leads to death. The main determinants (resulting from genetic predisposition and environmental factors) that characterize the aging process at the cellular level have been identified as: free radical damage; mitochondrial dysfunction results in an accumulation of reactive oxygen species (ROS) and consequent oxidative stress; decrease and inefficiency of autophagy (an evolutionarily conserved process of recycling and “cellular waste removal” that is essential for cellular integrity, more details a bit ahead); changes in hormone-related signaling processes such as type 1 insulin-like growth factor (IGF-1), insulin and growth hormone; change in cholesterol and glucose metabolism; telomere shortening (Testa et al., 2014).
Now it seems that the aging process is indeed multifactorial. Probably the various aging theories (see part 1) are correct! In general, molecular processes are becoming more inefficient, slower and the system is progressively moving towards entropy. However, it seems that knowing the autophagy process (whose decline is associated with aging) may offer a “new” perspective on aging. Autophagy (or “self-digestion”) has been defined as an evolutionarily conserved (normal and important) catabolic process characterized by degradation in the lysosomes (cell organelle that functions as a “litter”) of damaged organelles, “defective” proteins and intracellular pathogens (Lavallard et al., 2012). Autophagy provides macromolecule degradation and recycling, not only providing new nutrients and energy during energy restriction (during calorie restriction or fasting), but also preventing the accumulation of cell metabolism by-products and protein aggregates in the cytoplasm. Therefore, autophagy is a protective and essential process for cellular homeostasis (Rubinsztein, Mariño & Kroemer, 2011) (note: rest assured that autophagy will “eat all the muscles” for a few hours without eating. That simply does not happen!). In fact, several authors have pointed deficient autophagic capacity as an important mediator of cellular senescence and consequent occurrence of “diseases or characteristics of old age” such as cardiovascular and neurodegenerative diseases; oxidative stress; weak immune system; chronic inflammation; osteoporosis; sarcopenia; diabetes; obesity; cancer (Pallauf & Rimbach, 2013; Pyo, Yoo & Jung, 2013). Specifically, reviews of mechanistic animal studies have indicated that loss of function in autophagy-related genes has resulted in intracellular accumulation of defective proteins and organelles and consequently in the acceleration of aging, while promoting autophagic activity increased life expectancy (Yen & Klionsky 2008)
(Note: Autophagy mechanisms have been in the mainstream news since 2016 with the Nobel Prize in Medicine 2016 awarded to the Japanese biologist Yoshinori Ohsumi. Their findings in autophagy mechanisms point in the direction that this cellular cleaning and recycling process is essential to prevent neurodegenerative and other diseases. This is the LINK for the news article).
Overall, and since the first rat studies by Dr. Clive McCay in 1935, calorie restriction has been extensively reviewed and recognized as a “potent” anti-aging strategy! Interventions in various types of animal species (from invertebrates to larger mammals such as primates) have shown that calorie restriction (without malnutrition) not only increases life expectancy (average and maximum), but delays the onset of so-called “age-related diseases ”(Martin, Mattson & Maudsley, 2006; Xiang & He, 2011; Lee & Min, 2013; Kitada & Koya, 2013b; Szafranski & Mekhail, 2014; Testa et al., 2014). The intermittent fasting regime (nothing more than another calorie restriction strategy as described in part 1 of this article) seems to offer the same kind of benefits (Martin, Mattson, & Maudsley, 2006; Robertson & Mitchell 2013).
Now the mechanisms by which calorie restriction or fasting induce health benefits appear to be (to a large extent) related to this antagonistic relationship between insulin signaling and autophagy. It is easy to understand, being autophagy a catabolic process (essential, normal and protective, I highlight that again) and the activation of insulin signaling pathways an anabolic process (equally important and essential in protein synthesis, insulin is not the “villain”), when one of these pathways is activated the other will be inhibited. Practically speaking, fasting activates the autophagy “machinery” and eating a meal (mainly containing protein and / or carbohydrates) activates the insulin signaling “machinery”. What seems to be essential is in fact that there are periods that allow the process of elimination and recycling provided by autophagy, and for this to happen it is necessary not to eat for a while. If there is no “room” for this process, due to constant food intake, it may lead to constant and “aberrant” insulin signaling state which may lead to many diseases that are usually associated with poor glucose and insulin metabolism which make the most of the so-called “age diseases”.
(Warning: the “less nerds“ should skip next paragraph)
Briefly, some of the mechanisms identified in animal studies that appear to underlie the health benefits induced by caloric restriction or intermittent fasting through regulation of autophagy and insulin pathway signaling are: 1) Inhibition of insulin / IGF-1signaling (due to the decrease in circulating amino acids and glucose) and its target pathways protein kinase B (PKB) / mammalian target of rapamycin (mTOR) ; 2) Activation of the sirtuin 1 pathway (SIRT1) due to the increase in NAD + / NADH ratio, which targets include activation of adenosine monophosphate protein kinase (AMPK), forkhead box O (FOXO) transcription factors, proliferator- activated gamma receptor-1-alpha coactivator (PGC-1α) (a mitochondrial biogenesis factor), and inhibition of the pro-inflammatory transcription factor NFkB; 3) Activation of the AMPK pathway due to the intracellular increase of the AMP / ATP ratio, which in turn induces up-regulation of FOXO and PGC-1α transcription factors and inhibition of the PKB / mTOR pathway. (Martin, Mattson & Maudsley, 2006; Han & Ren 2010; Rubinsztein, Mariño & Kroemer, 2011; Yen & Klionsky, 2008; Xiang & He, 2011; Pallauf, & Rimbach, 2013; Pyo, Yoo, & Jung, 2013; Hu & Liu, 2014; Szafranski & Mekhail, 2014; Amigo & Kowaltowski, 2014; Testa, G. et al., 2014; Madeo et al., 2015).
In humans, despite the smaller abundance of randomized controlled trials (for the reasons mentioned in Part 1 of this article), several reviews of intervention and observational studies (Yen & Klionsky, 2008; Marzetti, E. et al., 2009; Han & Ren 2010; Robertson & Mitchell, 2013; Testa et al., 2013; Madeo et al., 2015; Fan et al., 2016) indicate that the putative health benefits induced by calorie restriction or intermittent fasting are based on the same mechanisms related to insulin pathway signaling and regulation of autophagy. Some pointed benefits include: longer healthy longevity; better lipid profile; controlled blood pressure; optimization of diastolic and systolic function; better homeostatic control of insulin and glucose; better sensitivity to insulin and glucose; lower incidence of neurodegenerative diseases; lower adiposity; better mitochondrial biogenesis in the skeletal muscle; higher antioxidant capacity; lower levels of ROS and oxidative stress.
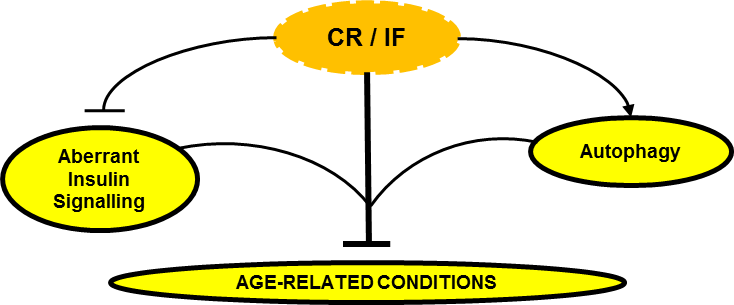
Can Calorie Restriction / Intermittent Fasting (CR / IF) alleviate age-related disease by regulating “aberrant” insulin signaling and autophagy?
In conclusion, the effect of caloric restriction or intermittent fasting on the regulation of insulin signaling and autophagy seems to emerge as a central regulatory axis that deserves attention (at least from me).
In the third part of this article I will then discuss what may be practical implications and applications of calorie restriction or fasting. Should we all do calorie restriction? Permanently? For how long? How much? What stage of life? Under what health conditions? Is the “intermittency” factor that delivers the best benefits?
Stay around!
Nuno Correia
References:
Amigo, I. & Kowaltowski, A.J., 2014. Dietary restriction in cerebral bioenergetics and redox state. Redox Biology, 2(1), pp.293–304.
Dröge W., 2009. Avoiding the First Cause of Death. New York, Bloomington. iUniverse, Inc.
Fan, J. et al., 2016. Autophagy as a Potential Target for Sarcopenia. Journal of Cellular Physiology, 231(7), pp.1450–1459. [Epub 2015 Dec 10].
Han, X. & Ren, J., 2010. Caloric restriction and heart function: is there a sensible link? Acta pharmacologica Sinica, 31(9), pp.1111–1117.
Hu, F. & Liu, F., 2014. Targeting tissue-specific metabolic signaling pathways in aging: the promise and limitations. Protein & cell, 5(1), pp.21–35.
Lavallard, V.J. et al., 2012. Autophagy, signaling and obesity. Pharmacological Research, 66(6), pp.513–525.
Lee, S.-H. & Min, K.-J., 2013. Caloric restriction and its mimetics. BMB reports, 46(4), pp.181–7.
Lee, S.-H. & Min, K.-J., 2013. Caloric restriction and its mimetics. BMB reports, 46(4), pp.181–7.
Lindeberg, S., 2010. Food and Western Disease: Health and Nutrition from an Evolutionary Perspective. Oxford, United Kingdom: Wiley-Blackwell.
Madeo, F. et al., 2015. Essential role for autophagy in life span extension. Journal of Clinical Investigation, 125(1), pp.85–93.
Martin, B., Mattson, M.P. & Maudsley, S., 2006. Caloric restriction and intermittent fasting: two potential diets for successful brain aging. Ageing research reviews, 5(3), pp.332–53.
Masoro.E. L., 2002. Caloric Restriction: A Key to Understanding and Modulating Aging. Texas, USA: ELSEVIER.
Pyo, J.O., Yoo, S.M. & Jung, Y.K., 2013. The interplay between autophagy and aging. Diabetes and Metabolism Journal, 37(5), pp.333–339.
Robertson, L.T. & Mitchell, J.R., 2013. Benefits of short-term dietary restriction in mammals. Experimental gerontology, 48(10), pp.1043–8.
Rubinsztein, D.C., Mariño, G. & Kroemer, G., 2011. Autophagy and aging. Cell, 146(5), pp.682–695.
Rubinsztein, D.C., Mariño, G. & Kroemer, G., 2011. Autophagy and aging. Cell, 146(5), pp.682–695.
Szafranski, K. & Mekhail, K., 2014. The fine line between lifespan extension and shortening in response to caloric restriction. Nucleus, 5(1), pp.56–65.
Testa, G. et al., 2014. Calorie restriction and dietary restriction mimetics: a strategy for improving healthy aging and longevity. Current pharmaceutical design, 20(18), pp.2950–77.
Xiang, L. & He, G., 2011. Caloric restriction and antiaging effects. Annals of Nutrition and Metabolism, 58(1), pp.42–48.
Yen, W.-L. & Klionsky, D.J., 2008. How to live long and prosper: autophagy, mitochondria, and aging. Physiology (Bethesda, Md.), 23(70), pp.248–262.

CAN CALORIE RESTRICTION OR INTERMITTENT FASTING HELP PREVENT “AGE-RELATED DISEASES” AND LIVE LONGER? – PART 1
Introduction
In this article I will look into the possibility of calorie restriction or intermittent fasting, which is just an alternative strategy to induce a caloric deficit, effective nutritional therapeutic strategies to prevent, alleviate or even eliminate some of the so-called “age-related diseases”, thus contributing for a better and longer life. It is important to note that most studies on the effects of calorie restriction or intermittent fasting (or intermittent calorie restriction) on life expectancy are mechanistic, and conducted in animal and / or in vitro models. It is understandable that there are fewer human intervention studies in this area. If we think about it, it is not easy to conduct studies with humans on calorie restriction to study its effects on life expectancy and the incidence of “age-related diseases”. Not only it is not easy to recruit people to voluntarily incur in a calorie restriction period, it is also not practical to study in humans (in a randomized controlled manner) the effects of calorie restriction or fasting on life expectancy, because they simply “live a long time”. ” In order to obtain timely results, it is essential to conduct studies on species with a shorter life expectancy. However, observational studies and some human intervention studies (discussed later) appear to confirm the same health benefits and molecular mechanisms as those observed in animals.
It should also be noted that, in the experimental context, caloric restriction is defined as “reduced food intake without malnutrition”. In other words, nutritional interventions imply a 10-40% reduction in daily caloric requirements in which only calories, and not nutrients, are restricted (in most controlled studies this is ensured with vitamin and mineral supplementation) (Kitada & Koya, 2013b; Robertson & Mitchell, 2013). This notion is important! Caloric deficit does not imply nutrient deficit and caloric surplus does not imply that nutrient requirements are met. Intermittent fasting will be no more than an alternative method of calorie restriction in which food intake is restricted for a certain period of time (usually 16 to 24 hours) followed by an unrestricted intake period and has been touted as producing beneficial health effects similar to more constant calorie restriction protocols (Martin, Mattson, & Maudsley, 2006; Robertson & Mitchell 2013).
Part 1
Should we accept being “sick” just because we get older?
It is recurrent to hear that the disease is something that “comes with the age package.” In fact, getting older is a drag! The general perception of a progressive decline of all our capabilities as we age is, unfortunately, not an illusion. There are several theories about aging. While certainly a very interesting topic, a detailed description of the various theories of aging is not the purpose of this article. These are some of mechanisms underlying the aging process which are generally pointed out as the main ones:
- The “Hayflick limit” (phenomenon discovered by Leonard Hayflick) determines that human cells have a replication limit number, after which they become senescent. Telomeres (i.e. a kind of protective “helmets” at the end of each chromosome) become progressively shorter with each cell division (Shay & Wright 2000). However, DNA methylation (an essential and repairing process consisting of the addition of methyl groups to DNA and which can be promoted by the abundance of dietary methyl donors for example) is said to be protective of telomere length and that way to postpone cell death and aging. For example, in animal models, hypomethylation of the enzyme telomerase reverse trancriptase has led to the preservation of leukocyte telomere length (Zhang et al. 2003; 2014). In this example, it is plausible to infer that delaying leukocyte senescence (through methylation and consequent telomere length conservation) may contribute to a stronger immune system and thus positively influence longevity.
- This theory suggests that unresolved chronic inflammation induces the human organism not to allocate resources for the functioning of other body functions (as they are permanently allocated to unresolved inflammation) and thus leading to early aging of various organs and tissues, and the early onset of “age-related diseases”.
- This theory, originally proposed by Dr. Denham Harman in 1956, is based on the premise that the aging process is mediated by free radical damage. Theoretically, by reducing free radical accumulation (e.g. reactive oxygen species) and at the same time increasing the antioxidant capacity of the organism (increasing glutathione, and antioxidant enzymes such as SOD and catalase), tissue damage can be prevented (by slowing down aging process) and to prevent the occurrence of “age-related diseases” and consequently contribute to increase functional longevity (Harman, 1988; 2006).
Very well, getting older is inevitable! We already know that. However, if we give it a little thought, all the mechanisms mentioned have an environmental root, that is, we can, to some extent, control them through decisions that we make every day. Namely decisions about what we eat and how we move. And this is good news! It is in fact in our hands to slow down the process of senescence and prevent the onset of the so-called ‘’age-related diseases’’. Note that if for us (Westernized world) it is statistically “normal” to grow old with diabetes, hypertension, cancer, dementia, sarcopenia, osteoporosis, cardiovascular disease, insulin resistance, obesity and chronic inflammation (because the population studied incurs in a lifestyle that leads to disease), in other contemporary (non-Westernized) populations such diseases are rare or even non-existent. In this context, I invite the reader to consult what I consider to be one of the best books I know about nutrition and lifestyle, and its relation to the incidence of so-called “Western” diseases: Food and Western Disease: Health and Nutrition from an Evolutionary Perspective by Staffan Lindeberg. In fact, if we want to aim at maximizing health and lifespan potential, we should not just look at what is ‘’normal’’ in a given population, because that may be a sick population. Rather, we should look for what is “biologically normal” for a human being! A species that is designed (evolutionarily) to deal with a range of environmental stimuli that include certain levels of physical activity, nutrition, sun exposure and sleep. And, although aging is a normal process, it should not be “biologically normal” to age with chronic disease.
In this context, the Okinawa Centenarian Study is also frequently cited. The Okinawan population has the highest ratio of (healthy) centenarians on the planet (50 / 100,000 vs 10-20 / 100,000 in the USA) and as such is of greatest interest to study the factors that potentiate this kind of longevity. One of the factors identified (in addition to an appreciable level of physical activity and social interaction) was the fact that populations over 70 eat about 11% of calories below (about 1785kcal / day, which is a very moderate level of calorie restriction) than would be recommended for maintaining body weight (according to the Harris-Benedict equation), however on a nutrient-rich diet (Wilcox et al., 2006).

What we can do to live longer and better is one of my main interests. As I mentioned, our choices regarding the type of exercise, food we eat and other lifestyle factors can affect how long we live and, perhaps most importantly, how healthy and functional we live. In Part 2 of this article I will discuss some mechanisms by which nutritional interventions such as calorie restriction or intermittent fasting can lead to health benefits. And in Part 3 I will address the possible implications and practical applications of the practice of calorie restriction or fasting, as well as which populations can benefit most from these nutritional strategies and whoshould avoid them.
Stay around!
Nuno Correia
References
Dröge W., 2009. Avoiding the First Cause of Death. New York, Bloomington. iUniverse, Inc.
Harman D., 1988. Free radicals in aging. Mol Cell Biochem. Dec; 84(2), pp.155-161.
Harman D., 2006. Free radical theory of aging: an update: increasing the functional life span. Ann N Y Acad Sci. May;1067, pp.10-21.
Kitada, M. & Koya, D., 2013b. SIRT1 in Type 2 Diabetes: Mechanisms and Therapeutic Potential. Diabetes & metabolism journal, 37(5), pp.315–25.
Lindeberg, S., 2010. Food and Western Disease: Health and Nutrition from an Evolutionary Perspective. Oxford, United Kingdom: Wiley-Blackwell.
Martin, B., Mattson, M.P. & Maudsley, S., 2006. Caloric restriction and intermittent fasting: two potential diets for successful brain aging. Ageing research reviews, 5(3), pp.332–53.
Masoro.E. L., 2002. Caloric Restriction: A Key to Understanding and Modulating Aging. Texas, USA: ELSEVIER.
Robertson, L.T. & Mitchell, J.R., 2013. Benefits of short-term dietary restriction in mammals. Experimental gerontology, 48(10), pp.1043–8.
Shay J.W., Wright W.E. 2000. Hayflick, his limit, and cellular ageing. Nat Rev Mol Cell Biol. Oct;1(1), pp.72-76.
Zhang D. et al., 2013. Homocysteine-related hTERT DNA demethylation contributes to shortened leukocyte telomere length in atherosclerosis. Atherosclerosis. Nov; 231(1), pp.173-179.
Zhang D.H., Wen X.M., Zhang L. & Cui W., 2014. DNA methylation of human telomerase reverse transcriptase associated with leukocyte telomere length shortening in hyperhomocysteinemia-type hypertension in humans and in a rat model. Circ J. 78(8), pp.1915-1923.
Wilcox D.C. et al., 2006. Caloric restriction and human longevity: what can we learn from the Okinawans? Biogerontology 7, pp.173–177.

Strength training has been recognized as the strategy of choice to stay more functional and live longer. The benefits of strength training are in fact ubiquitous and positively affect the various biological systems that tend to decline with age, namely systems related to neuromuscular, cardiovascular and cognitive functions.
It has been observed that strength training programs in which the included exercises are performed at higher intensities (> 80% of maximum intensity) or with lighter loads but performed explosively tend to produce better results compared to training protocols where exercises are performed at lower intensities and / or non-explosively (Mendonça et al., 2016a). The magnitude of the load used (i.e. heavy or lighter but performed explosively) are especially relevant for older populations. Why? Because aging is associated with the loss of Type II muscle fibers, which are responsible for producing maximal strength (e.g. lifting a weight and not being able to lift it again in the next minutes or hours) or as explosive strength (e.g. moving an object or your own bodyweight at maximal speed). Now, the overwhelming majority of daily life movements are ballistic in nature (i.e. fast, short duration movements) and often for the purpose of moving relatively heavy objects for a short period of time. Therefore, it is not surprising that a training program that includes exercises that imply moving heavy loads and / or loads moved explosively is more effective in “preparing” people for everyday activities.
Training at higher intensities in a training program based on fundamental movement patterns (squatting, pushing, pulling, loading and lifting objects off the ground) makes people less vulnerable to falls and “tweaks”, and at the same time more able to recover from such incidents should they occur.
Train hard and smart! A structured training program that respects the principle of progressive overload is more valuable than a program that always keeps you within the comfort zone. Be as active as you can get during the day but IF TRAINING AT GYM DO NOT WASTE YOUR TIME, AND REALLY TRAIN! Seriously, it works!
Good lifting! ?
References
Mendonca, G. V. et al., 2016a. Impact of Exercise Training On Physiological Measures of Physical Fitness in the Elderly. Current aging science, 9(3).

The self-reported prevalence of shoulder pain is estimated to be 16-26% and this is the third most common cause of musculoskeletal disorder on consultation (see reference below). Physical factors such as your exercise habits and repetitive (low and high intensity) movements in inappropriate positions can result in injury or chronic pain.
For these reasons, at The Strength Clinic, we consider that there are four fundamental pillars in the way your shoulder should function:
1) Breathing – Breathing properly is very important to maximize performance. A normal person breathes on average more than eight million times a year, and it is likely that he/she does not do it efficiently. Most people use only a small percentage of the body’s ability to draw oxygen from the air into the lungs because they tend to breathe only through the upper respiratory tract (apical breathing), instead of breathing deeper from the most efficient respiratory muscle we have, the diaphragm.
2) Posture – Although overrated most of the time, each individual’s posture may have an influence on the onset of injuries and in the prevalence of chronic pain. Especially when we talk about activities with high impact / high loads (in which biomechanics assumes a fundamental role) and the daily habits of movement that each person has. A poor posture is usually the result of various structural, muscular and joint imbalances. However, it should be noted that our body has a huge adaptive capacity and that the lack of quality movement is probably the main problem. Contrary to what you may think there are no perfect postures!
3) Grip Strength – There is a phenomenon called irradiation, so the higher the grip strength, the greater the activation of nerves and muscles along the kinetic chain. Therefore, there will be an increase in neurological efficiency, and we will have the rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis) firing the way they should, which is as dynamic stabilizers centering the head of the humerus on the joint, and not otherwise inhibited due to lack of grip strength. The hands are closely linked with the functioning of the physiological and neurological system but unfortunately this is a phenomenon largely ignored in today’s training programs.
4) Joint Position – Rotator cuff training alone will not ensure the functional health of your shoulder. The stability of the shoulder blades, which depends on the mobility of the thoracic spine, is critical to ensure that the glenoid cavity is well positioned for the applied forces. The stability of the hips and trunk is also necessary to serve as a foundation for the position and functioning of the shoulder blades. In other words, if your central axis control is weak, your shoulder blades are most likely to be drawn into unfavorable positions and this will impair force transmission.
Therefore, any strategy aimed at improving the functionality of the shoulder should consider these four pillars because a seemingly strong shoulder is not necessarily a stable shoulder and it is stability that must precede force production.
Pedro Correia
References
Mitchell C, Adebajo A, Hay E, Carr A. Shoulder pain: diagnosis and management in primary care. BMJ: British Medical Journal. 2005;331(7525):1124-1128.

For many years, breast cancer survivors have been told not to lift anything heavier than a handbag because of the risk of lymphedema (swelling / edema caused by accumulation of lymphatic fluid in the tissues of the body’s surface). This accumulation of lymphatic fluid (lymph) arises as a consequence of changes in the lymphatic system due to surgery and / or radiotherapy to the lymph nodes in the axilla and surrounding areas.
In this regard, it is recommended that women should ask for help with shopping bags, should avoid lifting or carrying children, and should only engage in exercise modalities such as walking, swimming and other light aerobic activities – these are the general recommendations. However, a study published in the New England Journal of Medicine in 2009 (see reference below) has shown that lifting weights can be a substantial aid to women with or at risk of developing arm lymphedema.
In this study the researchers recruited 141 breast cancer survivors with stable arm lymphedema and divided the sample into two groups – one group did strength training and the other did not change their exercise routine. These were the conclusions of the authors of the study: “in breast-cancer survivors with lymphedema, slowly progressive weight lifting had no significant effect on limb swelling and resulted in a decreased incidence of exacerbations of lymphedema, reduced symptoms, and increased strength.”
So, the main question here is not whether women who suffer from this condition may or may not lift weights but HOW they should do it to improve their condition. Again, the critical component is the program design, and this is one of our distinctive competencies at The Strength Clinic.
Train smart.
Pedro Correia
References
Schmitz KH, Ahmed RL, Troxel A, Cheville A, Smith R, Lewis-Grant L, Bryan CJ, Williams-Smith CT, Greene QP. Weight lifting in women with breast-cancer-related lymphedema. N Engl J Med. 2009 Aug 13;361(7):664-73. doi: 10.1056/NEJMoa0810118. PubMed PMID: 19675330.

Following up on the topic addressed in the last article, let’s talk today about a common swing characteristic that affects a lot of golfers and that can compromise their swing efficiency and their performance on the golf course: Early Extension.
What is Early Extension?
Early extension can be understood as an integral part of loss of posture, this happens when the player’s hip and spine begin to extend too early in the downswing, i.e. the hips and pelvis move towards the ball in the downswing. In practical terms, if your body is not prepared to perform an efficient golf swing while maintaining good posture throughout the movement, you will end up lifting the upper body (spine) and miss the necessary hip rotation at impact. Your hips play a key role in injury prevention and performance improvement. If you have poor hip mobility, sooner or later your lower back will complain (and you can be sure that this situation will not be very pleasant).
According to studies conducted by the Titleist Performance Institute, 64.3% of amateur golfers early extend
Players who early extend usually refer that they feel trapped during the downswing as if they had to shrug their arms to hit the ball. And it’s normal for that to be so because when you extend your hips too early on the downswing, the space that was supposed to be occupied by your arms and hands was occupied by the lower body. Therefore, the end result will be a blockage of the movement, since your arms and hands can’t get out of the way and will still be needed to hit the ball.
How can I diagnose?
An easy and simple way to check if you do early extension is with your Smart Phone (you probably already have applications that allow you to draw lines and analyze your swing). All you need to do is to ask a friend to film you in the direction of the swing line and capture its full motion from the starting position (setup). After having your swing recorded, compare the position of your pelvis in the initial position with the position of the pelvis in the position of impact, if you notice that it moved towards the direction of the ball is because you extended your hip too early. If this is not possible, you can always ask your golf teacher to help you, I am sure he will be happy to do that.
What are the physical limitations?
“If you’re not assessing, you’re just guessing” – Greg Rose
The physical limitations can be many and to determine the causes that are affecting you, it would be important to make a functional assessment with a professional who understands how your body should move and its relation to the golf swing. According to what I have observed in my practice, I would like to highlight the following:
- Limitations on performing a full squat with the arms extended overhead;
- Limitations in hip mobility (especially in internal rotation of the leading hip and in anterior or posterior pelvic tilt);
- Limitations in the ability to separate / disassociate the thorax from hips (X factor);
- Limitations in the ability to stabilize the pelvis because the glutes and core muscles are inhibited.
What can I do to improve?
Although the causes may vary from person to person, I’m pretty sure that if you do the following exercises, you will improve and increase your body’s functionality to play golf for a longer time. You only need 10 minutes a day.
- Myofascial Release with Roller Stick

Using a roller stick, look for the trigger points of your calf and massage the inner, central and outer sides of the muscle for 30 seconds in each area. The points that hurt you most are those that need more care. Yes, this exercise might be a little uncomfortable but it’s worth it.
- Glute Bridge with Leg Extension

Lying in the supine position, push your heels against the floor, tighten your glutes, and raise your hips to form a glute bridge, with your arms up. Once in this position, extend one leg and form a straight line between the shoulder, hip and heel. Hold this position for 20-30 seconds, always keeping your hips high. Change legs and repeat 5 times on each side.
- Squat with Overhead Arm Reach

In the squat position (with your heels on the floor and your knees out), raise one arm up, lift the other arm (always looking at your hand) and then raise both arms at the same time and return to the standing position. If you can not squat without raising your heels, you can use a rolled up towel or a board to keep your heels high. Do 2-3 sets and repeat 8-10 times.
- Assisted Squat wiht Medicine Ball

In the standing position, with your feet shoulder-width apart and slightly rotated out, hold a medicine ball (or a bucket full of balls) in front of your body, and begin to slowly lower your body into the squat position by keeping your back straight and without lifting your heels off the floor. Do 2-3 sets and repeat 10-12 times.
I believe that these exercises can be helpful to you, but remember: The swing you can do is directly related to what your body is prepared to do.
See you soon!
Pedro Correia

“Do not judge a man’s strength by the size of his biceps. Things do not always look what they seem.”
– Pavel Tsatsouline
In my opinion a normal human being should aim to be strong. And when I say strong, I’m not talking about those bulked individuals with a strange gait. Anyone (of any age) can become stronger by working consistently for this. Unfortunately, most people are more WILLING to be strong than doing what they need TO DO to be strong. Yes, these are different things. And yes, it’s not easy. One thing is WANTING a top-of-the-range Porsche, another thing is DOING the things needed to have a top-of-the-range Porsche. With strength is the same situation. To be strong, you need to have a plan (or have someone design a plan for you) and to work consistently to execute that plan – this is what your objective should be: to execute the plan. That’s it. You do not become what you THINK about every day, you become what you DO every day. Yes, there are no miracles, no one gets stronger without effort and without spending the time necessary for that to happen. The fitness magazines and the marketing associated with this industry want to make you believe that it’s possible to get stronger or leaner without great effort and quickly. It’s because of these kinds of messages that people still believe in shortcuts and / or allude to the power of genetics. They want it all but they don’t do anything (nothing useful at least). And then they still blame genetics!
There is one thing you should be aware of right now, strength is a skill. And in this sense, strength is the ability to generate more tension in muscles. And that is why strength is the basis for the development of speed, endurance and even flexibility. Like all skills, there are techniques or more appropriate ways to develop it. And that’s what I’m going to share with you. I will teach you some techniques for you to get stronger faster but this will only work if you apply them consistently in training. So, do them! Some of these techniques have already been used with me and with my clients / athletes, so I can assure you that they work and that they are scientifically proven, if that interests you as well. And before explaining them, I want to refer to Pavel Tsatsouline (I love reading his books), since he has been one of the individuals who has shared most of the “Russian secrets” of strength and one of the persons who have inspired me most in this journey. I hope I can meet him someday. Ready? Let’s do it!
- Irradiation
This one is easy, this one any five-year-old understands.
First make a bicep curl set of 5-6 repetitions with good form, keeping the elbow close to the body and without tilting the trunk back. You can use a dumbbell or a barbell. But a serious dumbbell, it’s not worth using Barbie and Ken-style dumbbells, let these tools for people to have fun in aerobic classes! After doing this set, rest for a few minutes and make the following changes: before doing the movement again, i) squeeze hard the dumbbell or barbell; (ii) squeeze your glutes as if you wanted to crack a nut with your buttocks and (iii) tighten your abs and imagine that Mike Tyson will punch you in the stomach.
If you can do these three things, you will realize that the weight will get lighter and you will be able to do a few more reps – in a better and safer way. The explanation is this: when you create tension at various points in the body this will increase total body stability (via the neural impulses produced by the contracting muscles) and this stability / force will irradiate (i.e. spread) to the neighboring muscles as if it were an electric current to start the engine. And the most interesting part lies on the fact that the strength of a particular muscle, for example the bicep, can be amplified if the neighboring muscles also help! Have you realized why in the union lies strength? The formula is simple: more tension = more stability = more force.
- Bracing
Who still does arm wrestling in school? I perfectly remember the times when I was in school and this was one of the games we did in during class breaks or when we had a hole in our schedule. I remember very well the agonizing look of my classmates when they were about to be defeated or their expression of jubilation when I let them gain advantage and then finished strong. Yes, this was fun at the time! And yes, most of the time I won ?.
I gave the example of arm wrestling because I think this is the best way to understand this phenomenon. Lets’ see: an individual who can generate more tension before squeezing his opponent’s hand will have a superior neuromuscular activation level and a clear advantage over an individual who only begins to squeeze when someone (the referee) gives the signal to begin the “combat”. According to Prof. Yuri Verkhoshansky, if we create a sort of pre-tension in the muscles before starting a dynamic contraction, this can lead to increases of up to 20% in performance! Now imagine the advantage you can have if you can apply this technique and if your opponent does not know about it.
Try this technique as follows. Do five normal push-ups and relax on the floor between reps. Then do another five and this time think about creating tension in the whole body, that is, think of squeezing your glutes and abs before pushing against the floor to come up. If you do this well, you will realize that you are much stronger than you thought. Therefore, the key to this technique is in creating tension in the whole body before counteracting resistance. If you do not create this tension before, you will remain weak. Do not be that person.

- Power Breathing
First, a few notes on breathing. Proper breathing is very important to maximize performance, a normal person breathes on average more than eight million times a year and it is more likely that he will not do it efficiently. If there was a movement pattern that you had to repeat 23,000 times a day, would you not make an effort to improve it? Think about this a little bit. Most people only use a small percentage of the body’s ability to extract oxygen from the air into the lungs because they tend to breathe only with the upper body (apical breathing), instead of breathing deeper by using the most efficient respiratory muscle we have, the diaphragm (I think we do not talk much about the diaphragm in fitness / bodybuilding magazines because this is an invisible muscle that will not really impress women). But the fact is that this daytime breathing will affect several things: your recovery ability, your anatomical structure, the functioning of your autonomic nervous system, and your cognitive ability. So, if we are talking about performance optimization, be sure to improve your breathing patterns as well.
Second, regarding power breathing, this technique consists of holding the breath during the various phases of lifting. For example, the legendary Bruce Lee used to say that in the martial arts the power of breathing was more important than body strength. In general, the effect of breathing patterns and intra-abdominal and intra-thoracic pressure on strength is strangely ignored or misunderstood by fitness professionals and some medical authorities. These authorities seem to forget that orthopedic injury is much more common than cerebrovascular injury. That traditionally taught breathing pattern of inhaling when we lower the weight (eccentric phase) and exhaling when we raise the weight (concentric phase) may be useful in some cases (and we can’t say that’s wrong) but it’s not the one you want to do when you want to generate as much tension / strength as possible in the muscles. Why? Because the increase in intra-abdominal and intra-thoracic pressure will boost muscle excitability (through the pneumo-muscular reflex) and it is this process that will guarantee more stability in the spine and that will amplify your strength. This is the most natural way to produce strength! Yes, your fitness instructor may have said that forced exhalation of air against the glottis (i.e. the Valsalva maneuver) is hazardous to your health and that you may have a stroke doing this. But is this assertion correct? Prof. Yuri Verkhoshansky and Dr. Mel Siff, two of the world leading authorities on strength training, say the following in this regard in the book Supertraining, one of the strength training bibles:
“For example, the Valsalva maneuver associated with holding breath has a vital role in increasing intra-abdominal pressure to support and stabilize the lumbar spine during heavy lifting… It has been corroborated on many occasions that stress on the spine is decreased during any movement against high resistance and that exhalation during lifting increases the risk of injury to the lumbar spine. Thus, it is unwise to follow popular medical advice that people must exhale during the effort”. The authors further add: “while this may be appropriate for patients with heart disease or hypertension, this same action performed by an athlete who is doing squats or heavy lifting overhead, can seriously compromise spine stability and safety”.
Got it? This means that any healthy person can and should apply this technique if they aim to get stronger and lift heavy loads in a safe way. People with hypertension and heart disease should be more cautious in this regard but please note: this is not to say that they can’t strength train, there are many other ways to develop strength. By the way, it is already well documented in the scientific literature that these people can and should do strength training to improve their condition!
- Successive Induction
Successive Induction, such as the Law of Irradiation we have seen above, is another of the Sherrington Laws exploited to the maximum by the Russians. According to this law, contraction of a muscle – for example, the triceps – will make your muscle antagonist – in this case, the biceps – stronger than normal. In the early 1980s scientists suggested that this technique had a disinhibiting effect and later confirmed that a strength training program that included pre-tensioning an antagonist muscle (i.e. successive induction) was more effective than a program of conventional training. And the most interesting thing is that these benefits were not only limited to an acute performance increase, but also resulted in long lasting strength improvements.
Do the following test. Grab a barbell or free weight and get ready to make a bicep curl set with a load that allows you to do 5-6 solid repetitions. Remember, hold your elbows close to your body and do not lean your trunk back. Do one set and count the number of repetitions you can do with good form. After resting for a few minutes, keep the same weight and do another set, but this time using this new technique. When you bring the weight up, apply the other techniques you already know (irradiation and bracing) and on the descent apply the technique of successive induction, “pulling” the weight down with the triceps. In this way, you will give the biceps some rest on the descent (by preventing them from locking the movement) and will allow the triceps to also have a more active participation in the movement. You should expect to be able to do one or two more reps this way!
Therefore, when applying this technique, you will have two engines controlling the movement. And because of the co-contraction of both muscle groups, this technique may also offer greater benefits in terms of joint stability since the stress on them will be reduced (note: do not forget to discuss this with your doctor if you have joint problems).
Finally, my advice to you is this: if you want to start lifting heavy loads safely begin applying these principles in training (if you can’t do this alone ask someone you know to help you) and enjoy learning one of the skills (i.e. strength) you will need most to optimize your health. And be patient, do not expect to learn all these things from one day to another – it takes time and practice, good practice of course.
See you soon!
Pedro Correia
References
Tsatsouline, P. (1999). Russian Strength Training Secrets for Every American. Dragon Door Publications.
Tsatsouline, P. (2003). The Naked Warrior. Master Secrets of the Super Strong – Using Bodyweight Exercises Only. Dragon Door Publications.
Verkhoshansky, Y; Siff, M.; (2009). Supertraining. Sixth Edition – Expanded Version. Ultimate Athlete Concepts.
Verstegen, M.; Williams, P. (2014). Every Day is Game Day. Penguin Group.

“As pessoas não decidem o seu futuro, as pessoas decidem os seus hábitos e os seus hábitos decidem o seu futuro.”
– F. M. Alexander
Há nove anos atrás (2010)1, o European Working Group on Sarcopenia in Older People (EWGSOP) publicou uma definição de sarcopenia que foi amplamente utilizada em todo o mundo e essa definição fomentou avanços na identificação e no cuidado de pessoas em risco ou com sarcopenia. Ficou definida como uma síndrome caracterizada pela perda progressiva e generalizada de massa muscular e força com risco de resultados adversos, como incapacidade física, pobre qualidade de vida e morte. Porque a relação entre massa muscular e força não é linear (a capacidade de gerar força não depende apenas da massa muscular), os critérios para o seu diagnóstico incluíam baixa massa muscular e baixa função muscular (i.e força ou performance física).
Depois de sabermos que, em 2016, a sarcopenia foi classificada como uma doença pela Organização Mundial de Saúde, conforme foi referido na primeira parte deste artigo, o EWGSOP22 actualizou a sua definição operacional e as várias estratégias de diagnóstico, considerando agora que a força muscular (medida através da força de preensão ou do teste de levantar-se da cadeira) é o principal parâmetro para medir a função muscular, ainda mais importante que a quantidade de massa muscular. Portanto, é neste contexto, que justificamos o título deste artigo e que reforçamos a importância de partilhar esta mensagem com todos os profissionais de saúde.
As implicações desta condição na saúde humana são várias e largamente conhecidas: aumento do risco de quedas e fracturas3,4; prejudica a realização das actividades da vida diária5; está associada com doença cardíaca6, doença respiratória7 e disfunção cognitiva8; menor qualidade de vida9; perda de independência10,11,12 e morte13. Em termos financeiros, os custos na saúde pública também já foram calculados em vários trabalhos. Num estudo de Janssen et. al.14, em 2004, os custos da sarcopenia nos Estados Unidos foram estimados em 18,5 biliões de dólares anuais, representando cerca de 1,5% dos custos totais na saúde. Num estudo realizado cá em Portugal no Hospital de Santo António no Porto e publicado em 201615, verificou-se que os custos de hospitalização associados à sarcopenia foram superiores em 58,5% para pacientes com idade inferior a 65 anos e em 34% para pacientes com idade igual e superior a 65 anos. Mais recentemente (2018), no Hertfordshire Cohort Study no Reino Unido16, verificou-se que os custos associados com a falta de força muscular foram estimados em 2,5 biliões de libras anuais.
No cenário actual, em que o fenótipo do envelhecimento doentio prolifera a olhos vistos em todas as nações industrializadas, em que doenças como a hipertensão, o cancro, a depressão, o alzheimer e a diabetes tipo II estão a acabar com a vida das pessoas, é fundamental adoptar medidas que visem a melhoria da função de cada indivíduo ao invés do diagnóstico de doenças e da administração de medicamentos que, além de não contribuírem para resolver este problema, poderão ainda agravar a sua condição. Sabemos que os problemas de saúde principais estão relacionados com a má alimentação, com a inactividade física, com a falta de sono, com o excesso de álcool, com a exposição ao tabaco e aos ambientes poluídos mas também com a falta de movimento de qualidade, de vigor e de força muscular.
Os benefícios do treino de força na saúde estão bem sustentados na literatura científica e os mais importantes serão porventura os seguintes: diminuição da pressão arterial; diminuição do risco de osteoporose e sarcopenia; melhoria do perfil lipídico; aumento da capacidade cardiorespiratória; prevenção e gestão de dores crónicas; aumento da sensibilidade à insulina; melhoria do bem estar e auto-confiança. Mais, já são vários os estudos17,18,19 que têm mostrado uma forte e consistente correlação entre o aumento de força e massa muscular com a diminuição da mortalidade, reforçando o facto que o declínio da força associado aos níveis de sedentarismo actuais e ao envelhecimento precisam de ser tratados. Logo, um programa de treino de força bem desenhado, que atenda à competência do indivíduo e que respeite os princípios do treino, vai melhorar todos os indicadores de saúde atrás referidos e ainda todas as qualidades físicas necessárias (força, potência, velocidade, agilidade, equilíbrio, coordenação, mobilidade, endurance) para a realização das actividades da nossa vida diária. São estes parâmetros da função física que estão actualmente sendo propostos como biomarcadores do envelhecimento nos seres humanos20.
Por consequência, a programação do treino é que será o factor determinante nesta equação. E se é certo que este processo requer o conhecimento imperativo das ciências do desporto, é preciso não esquecer que o mesmo também requer trabalho aplicado no terreno e arte na instrução. Em vez de andarmos tão preocupados em seguir as guidelines e procurarmos pelos resultados estatisticamente significativos, devemos sim preocupar-nos que a nossa abordagem seja relevante para a vida da pessoa. Porque nós trabalhamos com pessoas. Pessoas que têm limitações de tempo para treinar. Pessoas com diferentes responsabilidades familiares e profissionais. Pessoas que têm vidas diferentes umas das outras. Pessoas que têm uma série de problemas metabólicos e/ou ortopédicos que nenhum estudo randomizado controlado jamais conseguirá reproduzir! Sim, este é um processo complexo.
Finalmente, sabemos que um dos mecanismos responsáveis pela atrofia muscular, sarcopenia e envelhecimento é a apoptose, a morte programada das células e um processo fundamental no envelhecimento. Mas quando treinamos, comemos e descansamos adequadamente estamos a enviar um sinal ao nosso corpo para a criação de um ambiente anabólico, um ambiente que potencia a libertação de factores de crescimento e que suprime a apoptose. Ou seja, o treino de força é um factor de crescimento macroscópico que suprime a morte programada das células (i.e. apoptose) mas ao contrário dos medicamentos em que o aumento na dose significa mais doença e dependência, um aumento na carga (mesmo que reduzido) significa mais saúde, mais força e mais vigor. Desta forma, as decisões diárias caberão sempre a cada um: tratar o corpo como um Ferrari ou tratar o corpo como um carro de aluguer.
Pedro Correia
Referências:
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing 2010; 39: 412–23.
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jan 1;48(1):16-31.
- Bischoff-Ferrari HA, Orav JE, Kanis JA et al. Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos Int 2015; 26:2793–802.
- Schaap LA, van Schoor NM, Lips P et al. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: the longitudinal aging study Amsterdam. J Gerontol A Biol Sci Med Sci 2018; 73: 1199–204.
- Malmstrom TK, Miller DK, Simonsick EM et al. SARC-F: a symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J Cachexia Sarcopenia Muscle 2016; 7: 28–36.
- Bahat G, Ilhan B. Sarcopenia and the cardiometabolic syndrome: a narrative review. Eur Geriatr Med 2016; 6: 220–23.
- Bone AE, Hepgul N, Kon S et al. Sarcopenia and frailty in chronic respiratory disease. Chron Respir Dis 2017; 14: 85–99.
- Chang KV, Hsu TH, Wu WT et al. Association between sarcopenia and cognitive impairment: a systematic review and metaanalysis. J Am Med Dir Assoc 2016; 17: 1164.e7–64.e15.
- Beaudart C, Biver E, Reginster JY et al. Validation of the SarQoL(R), a specific health-related quality of life questionnaire for Sarcopenia. J Cachexia Sarcopenia Muscle 2017; 8: 238–44.
- Dos Santos L, Cyrino ES, Antunes M et al. Sarcopenia and physical independence in older adults: the independent and synergic role of muscle mass and muscle function. J Cachexia Sarcopenia Muscle 2017; 8: 245–50.
- Akune T, Muraki S, Oka H et al. Incidence of certified need of care in the long-term care insurance system and its risk factors in the elderly of Japanese population-based cohorts: the ROAD study. Geriatr Gerontol Int 2014; 14: 695–701.
- Steffl M, Bohannon RW, Sontakova L et al. Relationship between sarcopenia and physical activity in older people: a systematic review and meta-analysis. Clin Interv Aging 2017; 12: 835–45.
- De Buyser SL, Petrovic M, Taes YE et al. Validation of the FNIH sarcopenia criteria and SOF frailty index as predictors of long-term mortality in ambulatory older men. Age Ageing 2016; 45: 602–8.
- Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R. The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc. 2004 Jan;52(1):80-5.
- Sousa AS, Guerra RS, Fonseca I, Pichel F, Ferreira S, Amaral TF. Financial impact of sarcopenia on hospitalization costs. Eur J Clin Nutr. 2016 Sep;70(9):1046-51. doi: 10.1038/ejcn.2016.73. Epub 2016 May 11.
- Pinedo Villanueva, R. A., Westbury, L. D., Syddall, H. E., Sanchez, M., Dennison, E. M., Robinson, S. M., & Cooper, C. (2018). Health care costs associated with muscle weakness: a UK population-based estimate. Calcified Tissue International.
- Ruiz JR, Sui X, Lobelo F, et al. Association between muscular strength and mortality in men: prospective cohort study. BMJ. 2008;337(7661):a439. Published. doi:10.1136/bmj.a439.
- Srikanthan P, Karlamangla AS. Muscle mass index as a predictor of longevity in older adults. Am J Med. 2014;127(6):547-53.
- Dos Santos L, Cyrino ES, Antunes M, Santos DA, Sardinha LB. Changes in phase angle and body composition induced by resistance training in older women. Eur J Clin Nutr. 2016 Dec;70(12):1408-1413. doi: 10.1038/ejcn.2016.124. Epub 2016 Jul 13. PubMed PMID: 27406159.
- Cadore EL, Izquierdo M. Muscle Power Training: A Hallmark for Muscle Function Retaining in Frail Clinical Setting. J Am Med Dir Assoc. 2018 Mar;19(3):190-192.

Com o objectivo de melhorar as qualidades físicas de atletas, os autores são unânimes em afirmar que a força deverá ser vista como fundamental para a melhoria das restantes qualidades atléticas.
Como veremos ao longo do artigo, é considerado crucial tornar os atletas cada vez mais fortes, de forma a observar-se evolução no seu desenvolvimento atlético.
As diversas manifestações de força (força rápida e força de resistência) são influenciadas pela componente base, a força máxima, que é a capacidade do sistema neuromuscular produzir força contra uma resistência inamovível, independentemente do factor tempo (Mil-Homens et al, 2015).
A força muscular influencia as características força-tempo, que são importantes no desempenho desportivo pois, atletas mais fortes, apresentam mais força explosiva e taxa de produção de força. Ainda, segundo Suchomel et al. (2016), a capacidade de gerar força está directamente relacionada com a competência nas acções de potência muscular.
A força também influencia as acções desportivas relacionadas com a performance desportiva. Ser forte, implica conseguir efectuar acções de potência durante mais tempo e com intervalos menores de recuperação. Está directamente relacionada com a redução do número de lesões, devido à melhoria da qualidade nos ligamentos, tendões, cartilagens e tecido conjuntivo.
Influencia também a força relativa, que é o valor de força produzido por um atleta por unidade de massa corporal. Este conceito é fundamental em desportos nos quais os atletas têm de movimentar toda a sua massa corporal e competir por categorias de peso (Mil-Homens et al. 2015; Suchomel et al. 2016).
Por fim, a força também contribui para a melhoria das habilidades motoras gerais, como por exemplo, o salto, a corrida e as mudanças rápidas de direcção.
Pedro Ribeiro
(Artigo redigido no âmbito da prelecção “Treino Físico e Performance” no 9º Seminário – Desporto, Saúde e Cidadania, Março 2019.)
Bibliografia
- Bompa, T. O. & Haff, G. G. (2009). Periodization: Theory and Methodology of Training (5th). Human Kinetics.
- Joyce, D. & Lewindon, D. (Eds.) (2014). High Performance Training for Sports. Human Kinetics
- Mil-Homens, P., Correia, P. P. & Mendonça, G. V. (Eds). (2015). Treino de Força, Volume 1: Princípios Biológicos e Métodos de Treino. FMH Edições.
- Raposo, A. V. (2005). A Força no Treino com Jovens: Na Escola e no Clube.
- Suchomel, T. J., Nimphius, S. & Stone, M. H. (2016). The Importance of Muscular Strength in Athletic Performance. Sports Med, 46, 1419–1449. doi: 10.1007/s40279-016-0486-0.

“We don’t believe there is one way to swing a club; we believe there is an infinite number of ways to swing a club. But we do believe there is one efficient way for all golfers to swing a club and it is based on what they can physically do.”
– Titleist Performance Institute
If you’re reading this, you’re probably interested in improving your physical condition to make more birdies, hit longer drives, and increase your longevity as a golfer. Or, perhaps, your goal is to become the best player in your club or win the next Match Play Championship. No matter what your motivation is, the fact is that if your goal is to improve your game, this will require you to prepare yourself a bit better than most golfers I know. And better does not necessarily mean training longer hours!
If you´re still one of those players who spends hours and hours hitting buckets of balls on the driving range hopping that this will help you improve your golf game, you need to change your strategy. Hitting buckets of balls in the driving range and making chips and putts is not enough. If you truly want to improve your performance in this sport, your practice needs to include general athletic development exercises and specific physical training for golf, in a progressive and periodized manner.
This means that what you normally see in the gym has nothing to do with what you need to do to hit farther, straighter and to go through the 18 holes without getting so tired.
First: Is your swing efficient?
The only way to determine whether your golf swing is efficient or not is through a 3D Biomechanical Analysis. What we can see in the traditional video imaging used by most golf professionals / teachers is just the swing style. There are many golfers who do not have a particularly attractive swing (e.g. Raymond Floyd, Jim Furyk or John Daly) but the reason why these players were or are successful is because their swing is efficient. Having an efficient swing for a golfer means transferring energy (without leaks) through the feet, knees, hips, spine, shoulders, arms, wrists down to the club head and ultimately to the ball. With the data obtained through the 3D system, we can check the kinematic sequence of each player, that is, we can measure the speed of rotation of each body segment involved in the execution of the golf swing and determine if each segment is accelerating and decelerating correctly.
When we look at Jim Furyk and Ernie Els swing through video analysis (and through the naked eye), we can see that both swings are quite different from each other, however, when we look at the kinematic sequence of each player, we find that it’s difficult to see a significant difference between the two swings. This means that although Ernie Els and Jim Furyk have completely different swing styles, they both share the same kinematic sequence.
All great players start by generating speed from the hips and transferring that energy through the torso, arms and club. This is the efficient sequence in the downswing.
The golf swing is a complex multi-dimensional movement that involves a highly coordinated action of the entire kinetic chain (feet, knees, hips, spine, shoulders, arms and wrists) and takes less than two seconds. The golf swing is therefore a ballistic movement which, in order to perform efficiently (i.e. with a correct kinematic sequence), it’s necessary that the various body segments are properly prepared to deal with the inherent shear and rotation forces in this movement. Hence the importance of what follows.
Second: The Physical Assessment in Golf
Before we get to the physical training itself, it’s important to know what your physical limitations and asymmetries in terms of movement are (one of the main causes of injury). Because of this, it’s essential that you perform a functional assessment for golf, preferably with a qualified professional that knows what he’s doing. In the same way that you go to the doctor for exams to find out how your health markers are, you should also do an initial assessment with a golf fitness specialist to find out how your body behaves during a golf swing and which are the main limitations / compensations.
The physical evaluation in golf consists of performing several tests in order to measure the functionality of the body movement patterns necessary for golf, that is, the measurement of various indicators of its stability, mobility, balance and various performance parameters such as strength, power and cardiovascular capacity.
This type of assessment is the starting point for playing better and for preventing injuries. If you still think that your body is fine and that you don’t need any intervention at this level, you’re more likely to be wrong. Our body was not designed to lead the way we live today, so you can be pretty sure there are things in your body that need some work. If you still do not believe me, think of golfers you know who have never complained of back pain or pain in another part of the body (wrists, shoulders, elbow).
Your body is the determining piece of equipment in your game. The quality of the clubs, balls, gloves, shoes and the latest drive or putt on the market, are certainly not the most important aspects. I still see many golfers too preoccupied with the new gadgets and the style of clothing, when in fact these are not the most important things to get more birdies. What will, in fact, bring you better results is improving your body’s functional skills to hit the ball more efficiently and safely.
Final Remarks
Many players fail to perform an efficient golf swing not only because the movement itself is complex but also because their bodies are not properly prepared to deal with the forces generated during the movement.
Keep this in mind the next time you hit balls or have a lesson with your golf teacher, maybe that’s why you can’t do what your teacher asks you to do. There is no point constantly insisting on improving technique if there is no synergistic effort in improving physical skills. The swing you can perform is directly related to what your body is prepared to do – think of the golf club as an extension of your body.
In the next articles I will share the most common characteristics in this relationship between the body and the golf swing and suggest some exercises so that you can improve your performance on the golf course.
Stay tuned!
Pedro Correia

If you still exercise to “burn calories,” you have not yet realized the purpose of a physical training program and the importance that movement has in our lives. The least important thing about exercise is the number of calories you burn! And that’s what I’ll try to explain in this article.
The power of exercise goes far beyond calorie burning, caloric expenditure is just a (nice) side effect of the type of exercise we do. Exercise consists of potentiating the release of powerful molecules and hormones that “talk” to our body’s organs (it’s not just food that has this kind of influence), and that determines what’s going to happen. And usually, the higher the intensity, the more beneficial the hormonal response.
Therefore, a well-designed physical training program has more to do with increasing energy levels, movement precision, vigor, muscular strength, mobility, agility, speed, work capacity and with an improved hormonal profile.
The Calorie Fever
I still see a lot of people worried about the calories in their food, the calories they burn when they exercise, the calories they consume each day, and I ask: How did we get here? What kind of message is being propagated that made people so obsessed with calories? Is calorie counting that important? Let’s see.
In order to discover the amount of energy in food, scientists burn food samples in a bomb calorimeter. And, to my knowledge, a bomb calorimeter does not share the same physiology and genetic makeup as a human being. As far as I know, a bomb calorimeter does not depend on the functioning of the various systems in the human body which are the real players in the way energy is absorbed and used (examples: digestive, endocrine and nervous system). This way of thinking is most likely unsustainable and ineffective long-term. This way of thinking is too reductive and does not solve the main problem – people’s lack of education regarding the importance of what we eat throughout our lives. Is it just me who finds it strange that most people are more concerned about their cell phones, cars and computers than with the origin and composition of the food they eat?
In fact, just look around and you’ll acknowledge that this is not the path to follow!
It is true that if we have the goal of losing fat mass, we must create an energy deficit, that is, the balance between the amount of calories (energy) entering our body and the amount of energy (calories) burned, must be negative. That’s the number one rule in rigid weight loss programs and that’s why we see Biggest Loser contestants training several times a day.
(Note: I should remind you that the Biggest Loser is a contest in which the goal is to lose weight in the shortest time possible, it’s not a contest to see who gets out of there healthier – if this was the goal probably there was no audience).
However, there is a lot more to be said. There are good calories and bad calories. The foods we eat, besides having a certain number of calories (which can be very difficult to determine with accuracy and can be highly variable), also have different properties with respect to their composition of macronutrients (protein, fat, carbohydrates) and micronutrients (minerals, vitamins, phytochemicals). These bioactive properties and compounds are what makes the difference and what should be studied preferentially. In my way of looking at things, it is more logical to first check the functionality of food (i.e. how its nutrients work) and then look at its caloric density, which can also be more or less functional depending on the objectives, morphology and specific conditions of each individual.
(Note: If you still think low fat diets are the most suitable for weight loss check the following study published in 2003 in the New England Journal of Medicine here, where it was shown that people on a high-fat diet lost more weight as those on a low-fat diet, the diet generally recommended by leading health organizations. But, of course, adherence to the diet will be the most important factor).
Back to calories…
Because the absorption of these nutrients will depend on the functioning of our digestive system – which in turn is governed by the endocrine system (think of hormones) and the nervous system (think of neurotransmitters) – and the health of the organs involved in the digestion process (mouth, esophagus, stomach, pancreas, small intestine, large intestine, liver, gallbladder), it becomes easy to understand that the web of relationships in the human body is much more complex than simple calorie counting. Albert Einstein has a quote that fits perfectly here: “make everything as simple as possible, but not simpler.”
The Power of Exercise
Anyone that is minimally informed about exercise already knows that long distance aerobic training is not the best choice for improving body composition and may even have opposite effects (catabolic effects) due to the pronounced increase in cortisol levels.
This has been known for a long time but it’s always important to remember. This study published by Tremblay, Simoneau and Bouchard in 1994, showed that the group that did 15 weeks of interval training burned NINE TIMES more fat than the group that did aerobic training. And this was in half of the time period!
What you need to “burn calories” is to increase the intensity of your workouts for certain periods of time, it’s this type of stimulus that will increase your metabolism and accelerate fat loss. In this study, a 30-minute training session of metabolic resistance training caused a 38-hour increase in metabolism – the famous afterburn effect or EPOC (post-exercise oxygen consumption). Let’s put this into perspective. Let’s say you trained this way on Friday morning. With this training method your body will still be in a “fat burning” mode on Saturday night, when you’re having dinner with your friends or with your boyfriend / girlfriend.
And why do I insist on combining a good diet with good training? Because I’m aware of the evidence on this topic. This study from 1999 showed that those who did aerobic training and strength training on a low calorie diet burned 44% more fat than those who merely followed dietary guidelines. As I’ve been saying, diet is the most important component for those people who want to lose fat, however, once that aspect is assured, only strength training and interval training can actually bring your results to a higher level. In my opinion, the fact that this study was based on a low-calorie diet combined with aerobic training is limiting, but we have to bear in mind that these are usually the guidelines of the American College of Sports Medicine (ACSM). The guidelines are intended to facilitate nutritional guidance offered by practitioners, but unfortunately that is not what I have observed when I discuss these issues with some colleagues.
I think you have already realized that the type of training you do can be a great ally to put your body in an energy deficit and consequently in fat burning status. Now I will try to explain why this is the least important of all. Stay with me!
Like nutrition, physical exercise is key to improve health, performance and body composition. You’re probably tired of hearing this. But it’s not any kind of physical exercise that works. Doing hundreds of crunches to lose belly fat, using all the gym machinery, running 10 miles a day, doing Pilates twice a week and doing 100 power cleans in the shortest time possible is not enough. You can call it physical exercise if you want, but it’s not just this kind of physical exercise our body needs. A more comprehensive approach is needed.
We need Good Movement (we shouldn’t start running in the first place)
The concept of “move more for your health” is insufficient for our real needs and to improve quality of life. We need good movement, we need to acquire movement competency in the first place. I am talking about the ability to perform fundamental movements with good form. Fundamental movement patterns such as squatting, hinging, pushing, pulling, throwing, carrying, walking, running and jumping.
From my point of view, running should be the last step in this process and yet what we most frequently see is people running all crooked and with an obvious deficit in muscle strength. But the problem is not theirs, they are trying to do something for their health (and probably that’s all they know), the problem is that most of them are not aware that running is a skill, which requires preparation, practice and training. Cristiano Ronaldo did not become the best player in the World over night, it took many hours of training (in the field and in the gym) to reach this level. Although it’s relatively easy and affordable for anyone to put on their shoes and just go out for a run, running also requires preparation, practice and training (technical and physical).
It is necessary to have stability, mobility, strength (every step we take on the ground is subject to the action of gravity and the speed we run, generating reaction forces of 2 to 5 times our body weight), symmetry, quality of movement and good musculoskeletal health. Running to get healthy or fit is one of the greatest physical distresses on our body if we don’t have a solid foundation. First, you need to be in good shape to run. If you don’t hone good movement skills, you are more likely to get injured. According to the available literature, the incidence rate of injury in runners may exceed 90%, this is more than any other sport. Plantar fasciitis, stress fractures, patellar tendonitis and patellofemoral pain are just a few examples. Check this systematic review if you’re interested in learning more.
Again, don’t get me wrong, I’m not anti-running and I admire the effort and suffering capacity of all runners. I think we should all be able to run (by the way, that’s how we evolved as a species), the problem is that most people who run are not properly prepared to run and there are fundamental learning steps that should not be overlooked in order to prevent structural imbalances in the musculoskeletal system and injuries. Cleary the simplistic idea of “move more” is not enough.
A new way to look at training
Different types of training can affect the way our genes work and how they interact with our cells. With good training it’s possible to decrease chronic inflammation, improve insulin sensitivity, strengthen the cardiovascular system, improve lipid profile, slow down normal aging, burn fat (as we’ve seen in more detail above), increase confidence and self-esteem, increase energy levels, increase mental strength, improve a number of physical skills that we need for our daily life activities or sports practice (such as strength, stability, mobility, balance, speed, agility) and our different energy systems (ATP-CP, glycolytic, and oxidative). As we age, these skills naturally decline, but the fact is that with a more comprehensive training program it is possible to reverse and / or at least mitigate this decline.
Most people think that genes are the brain of the cell, they believe that if genes don’t tell you what to do, the cell dies. But if you remove the genes from the cell, the cell is still alive, eliminating waste products and behaving just like another cell. So, instead of genes being the brain of the cell, think of genes as your instruction / repair manual. When a worn part of the cell needs to be repaired or when new substances need to be produced, genes will give instructions for doing so.
Every cell in our body is surrounded by a fatty membrane, which is filled with thousands of receptors. These receptors receive information from different parts of the body and pass this information into the cell to form / encode new proteins, burn more or less fat, etc. (Note: this is why it’s important to eat good fats and avoid the hydrogenated fats present in most processed foods so that the cell membrane is more permeable to nutrient delivery.) It’s this membrane with receptors the cell command center so if we remove these membrane receptors, the cells die. This means that cell function is highly influenced by external factors, namely through hormones and other molecules that bind to these receptors.
These messenger molecules are not randomly created by our body, they are created according to our lifestyle, diet, thoughts, behaviors, temperature, light, sound and… our type of training. It’s possible to be born with some defective genes – for example BRCA 1 and BRCA 2, which increase the risk for breast cancer – but it’s these messenger molecules / hormones that will determine the degree of activation of these genes. Therefore, controlling these hormones means controlling the body.
(Note: Don’t you find it strange that almost 90% of health care costs is related to treat health conditions, while 80% of health problems / diseases arise as a consequence of our lifestyle and the environment we’re exposed to? Check this TED talk from Dan Buettner to realize why we are walking in the wrong direction).
High-intensity exercise is the one that induces a more favorable hormonal environment, with an increase in hormones such as testosterone, growth hormone and IGF-1, interleukins with an important role in inflammation (IL-6), muscle tissue maintenance (IL-15) and growing of new blood vessels (IL-8), lactic acid (which has the ability to keep us young by stimulating the release of testosterone and growth hormone) and nitric oxide, a vasodilator which plays a key role in regulating blood pressure, muscle strength and erectile dysfunction. Unfortunately, long running does not produce the same effects. Compound movements, which require a combination of strength and stamina, in short periods of time, are those that will put your muscles to “talk” more with your body. Burning calories is only a minor side effect when compared to the amount of hormones and other signaling molecules that influence how our body works.
To be clear, we are talking about intensity coupled with movement quality. Intensity coupled with bad movement will have the opposite effect: INJURY.
Conclusion
It’s urgent to give rise to a new mentality on training the movement skills that we will need throughout our lives. And this is a serious limitation of most group classes in conventional gyms. The instructors are obliged to follow a certain beat and choreography. Individualized feedback is almost non-existent. People don’t have time to understand or to learn the movements. And no one learns anything if they don’t know what it’s for, no one learns anything if they don’t understand how it’s supposed to feel and its practical implications. In addition, most machines in gyms annihilate the sensory and body perception that we, humans, need. We live in a three-dimensional world, in a world of constant adaptation and spatial exploration, so it makes no sense that machines and choreographies of group classes dictate the rules of our movement.
And why is it important to learn efficient movements? First, an efficient movement happens when a body is able to produce force through a coordinated action between the various body segments without energy leaks and demonstrating a natural ability to exploit maximum range of motion. Second, it’s movement that will allow you to play more time with your children, change the furniture at home, improve your day-to-day performance and your performance in your recreational activities.
Look at this type of training as the foundation, the support you need to get stronger, faster, smarter, more agile, more competent in a series of physical attributes that will allow you to perform better in the activities you enjoy doing. Would you like to start playing tennis? golf? volleyball? Would you like to start surfing? paddle board? weightlifting? powerlifting? dance? climbing? triathlon? Would you like to be faster when you play football with your friends during on weekends? Obviously, each modality has its specific abilities, but they all share the same foundation: human being’s adaptability capacity. To improve these specific skills safely, you first need to improve your fundamental movement patterns. And to sustainably keep improving these fundamental movement patterns, you need to train better and respect the developmental stages of each one.
To sum up, the great advantage of better training (and I remind you what we learned about the power of exercise, good movement and a new way of looking at training) is to improve your quality of life, maximize your performance and, above all, giving you the freedom and autonomy to choose the activity / sport that you always wanted to try but never had the courage or opportunity to start off.
Think about these things next time you go to the gym to walk on the treadmill with your headphones on and watch some TV series for 40 minutes while looking at the calories burned on the monitor and at the workouts or exercises other people are doing.
See you soon!
Pedro Correia
References
Berardi, J, Andrews, R. The Essentials of Sport and Exercise Nutrition. Certification Manual. Second Edition. Precision Nutrition Inc. (2013).
Björntorp P. Hormonal control of regional fat distribution. Hum Reprod. 1997 Oct;12 Suppl 1:21-5. Review.
Frederick F. Samaha, M.D., Nayyar Iqbal, M.D., Prakash Seshadri, M.D., Kathryn L. Chicano, C.R.N.P., Denise A. Daily, R.D., Joyce McGrory, C.R.N.P., Terrence Williams, B.S., Monica Williams, B.S., Edward J. Gracely, Ph.D., and Linda Stern, M.D. A Low- Carbohydrate as Compared with a Low-Fat Diet in Severe Obesity. N Engl J Med 2003; 348:2074-2081.
Gary D. Foster, Ph.D., Holly R. Wyatt, M.D., James O. Hill, Ph.D., Brian G. McGuckin, Ed.M., Carrie Brill, B.S., B. Selma Mohammed, M.D., Ph.D., Philippe O. Szapary, M.D., Daniel J. Rader, M.D., Joel S. Edman, D.Sc., and Samuel Klein, M.D. A Randomized Trial of a Low-Carbohydrate Diet for Obesity. N Engl J Med 2003; 348:2082-2090.
Houston, M. What your doctor may not tell you about Heart Disease. Grand Central Life & Style (2012).
Kraemer WJ, Volek JS, Clark KL, Gordon SE, Puhl SM, Koziris LP, McBride JM, Triplett- McBride NT, Putukian M, Newton RU, Häkkinen K, Bush JA, Sebastianelli WJ.
Influence of exercise training on physiological and performance changes with weight loss in men. Med Sci Sports Exerc. 1999 Sep;31(9):1320-9.
Schuenke MD, Mikat RP, McBride JM. Effect of an acute period of resistance exercise on excess post-exercise oxygen consumption: implications for body mass management. Eur J Appl Physiol. 2002 Mar;86(5):411-7. Epub 2002 Jan 29.
Tremblay A, Simoneau JA, Bouchard C. Impact of exercise intensity on body fatness and skeletal muscle metabolism. Metabolism. 1994 Jul;43(7):814-8.
van Gent RN, Siem D, van Middelkoop M, et al Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review British Journal of Sports Medicine 2007;41:469-480.
Existe atualmente evidência científica suficiente para afirmarmos que o treino de força é um método eficaz ao nível da prevenção, tratamento e, potencialmente, da reversão de várias doenças crónicas. Efectivamente, a adesão a um programa de treino de força devidamente desenhado pode aumentar de forma significativa a saúde física e mental da população.
A importância é tal que são várias as organizações de renome mundial (Organização Mundial de Saúde, Centers for Disease Control and Prevention, American Heart Association, American Association for Cardiovascular and Pulmonary Rehabilitation, American College of Sports Medicine) que recomendam esta forma de treino para manter a saúde.
No entanto, apesar desta evidência, a maior parte da referenciação para o exercício é ainda o treino aeróbio e são poucos os médicos (e profissionais de saúde em geral) que fazem a referenciação para o treino de força. Este artigo tem como objectivo alertar para a relevância e para o impacto valioso do treino de força na saúde.
Cerca de 100% da nossa existência biológica tem sido dominada pela actividade outdoor. Caçar e procurar comida tem sido uma condição da vida humana durante milhões de anos1. Ou seja, se no passado era preciso fazer esforço (i.e. actividade física) para encontrar comida hoje em dia a comida vem ter connosco sem ter que fazermos esforço nenhum. Portanto, passamos de um estilo de vida bastante activo para um estilo de vida altamente sedentário. Com consequências graves ao nível da saúde pública. Se antigamente todas as pessoas tinham que exercer algum esforço físico para fazer a sua vida normal hoje em dia a maior parte não tem essas necessidades. O ambiente mudou e as pessoas também mudaram. Estão mais fracas, mais doentes, têm mais dores crónicas e estão cada vez mais dependentes de medicamentos. Mas a mensagem que ainda se passa na nossa sociedade (e em consultas médicas) é “não faça esforços e faça a sua vida normal”. E eu acredito que este é o pior conselho que se pode dar às pessoas! A vida normal? Mas que conselho é este? Como é que o normal pode ser bom? É preciso estar completamente alienado da realidade para poder fazer recomendações deste género.
Hoje em dia temos mais oportunidades do que nunca para construir um fenótipo saudável e forte. O fenótipo é a expressão do nosso organismo e este, depende em grande parte, das escolhas que fazemos todos os dias. Dois organismos podem ter o mesmo genótipo, o mesmo DNA, mas diferentes fenótipos – baseado nas suas experiências e no ambiente. É certo que há coisas que não conseguimos controlar como a nossa herança genética, o local do Mundo onde nascemos / vivemos, a sorte e o ambiente. Mas há muitas coisas que conseguimos controlar e que depende exclusivamente das nossas prioridades na vida e das nossas escolhas diárias (exemplos: hábitos de exercício, alimentação, sono, gestão do stress, tabagismo, álcool, exposição a ambientes poluídos). E eu acredito que o exercício físico em geral (e o treino de força em particular) é o factor mais importante de todos. É o mais potente, é quantificável e actua rapidamente em todos os sistemas e orgãos do corpo humano.
A realidade é esta: a população está envelhecida e com mais doenças crónicas / não transmissíveis. As principais doenças não transmissíveis são as doenças cardiovasculares, cancros, doenças respiratórias crónicas e diabetes. Só estes quatro grupos de doenças contam mais de 80% para as 41 milhões de mortes no Mundo2! De acordo com o primeiro relatório sobre envelhecimento saudável da Organização Mundial de Saúde (OMS) espera-se que o número de pessoas com mais de 60 anos duplique em 20503 e é neste contexto que precisamos de intervir com urgência no sentido de promover a autonomia motora e melhorar a capacidade funcional das pessoas. As tradicionais recomendações das caminhadas, da natação, do Pilates e de “fazer esforços de baixa intensidade” ou “não fazer esforços” provavelmente precisam de ser reconsideradas e devidamente contextualizadas.
É neste âmbito que o treino de força e o treino das qualidades físicas assumem um papel lapidar. Todas as pessoas (atletas e não atletas) precisam de treinar as suas qualidades físicas para viver com qualidade e de forma independente. Depois dos 30 anos de idade, os adultos perdem 3-8% da sua massa muscular por cada década. Ao longo do tempo, a perda de massa magra contribui para uma diminuição da força muscular e da potência, importantes preditores de equilíbrio, da ocorrência de quedas e de mortalidade4. No caso dos idosos é importante assinalar que as quedas são a principal causa de morte acidental após os 65 anos e são as fracturas das ancas aquelas que afectam em maior extensão a independência dos mesmos5.
Quando falo em força refiro-me à base para interagirmos com o ambiente à nossa volta, à fundação para o desenvolvimento das outras qualidades físicas (mobilidade, potência, velocidade, agilidade, endurance muscular), à capacidade de produzir força contra uma resistência externa (pode ser o chão ou outro objecto qualquer) através das contracções musculares. Esta é, provavelmente, a capacidade mais treinável que dispomos e aquela que poderá ter maiores repercussões na melhoria da nossa função, na nossa independência e na nossa longevidade funcional. Tarefas como caminhar rapidamente, sentar e levantar de uma cadeira, subir escadas, manter o equilíbrio, carregar malas ou brincar com os filhos / netos, são exemplos de actividades da nossa vida diária que requerem uma componente mínima das várias manifestações de força (força máxima, força rápida e força de resistência). Portanto, tanto a força como o músculo (mais a sua qualidade que quantidade), são parâmetros da função física que precisam de ser cuidados na construção do fenótipo do envelhecimento saudável.
Estas questões assumem maior importância ainda quando constatamos que a partir do passado dia 1 de Outubro de 2016, na décima revisão da classificação internacional de doenças (ICD-10), a sarcopenia foi classificada como uma doença pela OMS sendo detentora de um código próprio (M62.84). Isto deverá levar a um aumento na disponibilidade de ferramentas de diagnóstico e a um maior entusiasmo da indústria farmacêutica para desenvolver medicamentos para combater a sarcopenia6. Mas na minha opinião isto também representa uma grande oportunidade para os profissionais do exercício poderem ajudar no combate desta doença, já que será o treino de força (devidamente orientado como é óbvio) o estímulo mais potente na sua prevenção e tratamento.
Pedro Correia
Referências:
- Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Comprehensive Physiology. 2012;2(2):1143-1211. doi:10.1002/cphy.c110025.
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet, 2016; 388(10053):1659-1724.
- Beard JR, Officer A, de Carvalho IA, et al. The world report on ageing and health: A policy framework for healthy ageing. Lancet 2016;387:2145e2154.
- English KL, Paddon-Jones D. Protecting muscle mass and function in older adults during bed rest. Current Opinion in Clinical Nutrition and Metabolic Care. 2010;13(1):34-39. doi:10.1097/MCO.0b013e328333aa66.
- National Center for Injury Prevention and Control of the Centers for Disease Control and Prevention. Preventing Falls: A Guide to Implementing Effective Community-Based Fall Prevention Programs 2nd edition. Atlanta: 2015.
- Anker SD, Morley JE, von Haehling S. Welcome to the ICD-10 code for sarcopenia. J Cachexia Sarcopenia Muscle. 2016 Dec;7(5):512-514. Epub 2016 Oct 17. PubMed PMID: 27891296; PubMed Central PMCID: PMC5114626.

A posição da mão no chão é um aspeto pouco considerado mas de grande importância para a qualidade do movimento. Nos últimos anos tem-se acentuado a prática de exercícios que exigem uma função de suporte por parte da mão (Exemplo: Handstand, Push-Up, Turkish Get-Up e muitas variantes de Crawling).
Em termos biomecânicos a mão desempenha um papel semelhante ao pé quando desafiada a suportar carga. Assim como o pé, o joelho e a anca interagem reciprocamente, as mãos interagem com a mesma reciprocidade em relação aos cotovelos e ombros. Dessa forma é necessário encontrar um equilíbrio de distribuição da carga de forma a otimizar a biomecânica da articulação com a necessidade do cérebro expressar uma exploração sensorial através de diferentes orientações da mão.
Numa perspetiva de desenvolvimento humano a aquisição de padrões motores grosseiros e rudimentares, como “sentir o chão”, precedem padrões mais refinados de controlo de objetos e realização de habilidades de alimentação, escrita ou gestos desportivos específicos. Se olharmos para o homúnculo humano rapidamente percebemos o papel que as mãos desempenham em nos conectar com o mundo e a importância da interação mão-chão.
Uma boa distribuição da carga ocorre quando existe uma dispersão de forças equilibrada entre toda a superfície palmar, sobretudo entre a região tenar e hipotenar. No entanto, a maioria das pessoas tem dificuldades em adotar uma posição de suporte correta principalmente se tiver de ser adotada de forma reflexa. A distribuição insuficiente ocorre quando as forças incidem maioritariamente sobre a região ulnar em detrimento da região tenar, causando uma sobrecarga desequilibrada sobre o punho. Um padrão de suporte insuficiente está correlacionado com os desequilibrios musculares cruzados na parte superior do corpo designados por Síndrome Cruzado Superior (Upper Crossed Syndrome). Descrito pelo Dr. Vladimir Janda como rigidez do trapézio superior, grande peitoral e elevador da omoplata e inibição dos romboides, grande dentado, trapézio médio e inferior e flexores profundos do pescoço, especialmente os músculos escalenos. O estereótipo das alterações posturais manifestam-se pela elevação e protração dos ombros, elevação das omoplatas, protração da cabeça e pela consequente instabilidade de toda a cintura escapular.
Um estudo realizado pela Dra. Alena Kobesova (2015) associou o efeito de exercícios de estabilização escapular, no qual um dos requisitos era a adoção de uma correta posição de suporte, com ganhos significativos na força de preensão.
Por sua vez, a força de preensão exerce um papel importante no bom funcionamento do membro superior, evidenciando que níveis mais elevados estão correlacionados com uma estabilização do ombro mais eficiente através de conexões neurológicas, aumento da transferência de força e diminuição da incidência de lesões.
Assim, adotar uma posição de suporte mais vantajosa contribui para um reportório motor mais rico no seu global.
Utilizamos a expressão “os pés bem assentes no chão” associada muitas vezes a uma tomada de decisão segura… Parece que ter “as mãos bem assentes no chão” também é positivo!
Patrick Filipe
Referências:
Kobesova. A, Dzvonik. J, Kolar. P, Sardina. A, Andel. R. (2015). Effects of shoulder girdle dynamic stabilization exercise on hand muscle strength. Isokinetics and Exercise Science 23 (2015) 21–32
Kolar. P, et. al. (2014). Clinical Rehabilitation. First Edition.
National Conference & Exhibition Bridging The Gap 2016. Grip Strength: Unleash the secret to primal strength, injury prevention, and overall health. Dr. Arianne Missimer.
Sacrey. LA, Whishaw. I. (2010). Development of collection precedes targeted reaching: resting shapes of the hands and digits in 1-6-month-old human infants. Behavioural Brain Research 214(1):125-9.
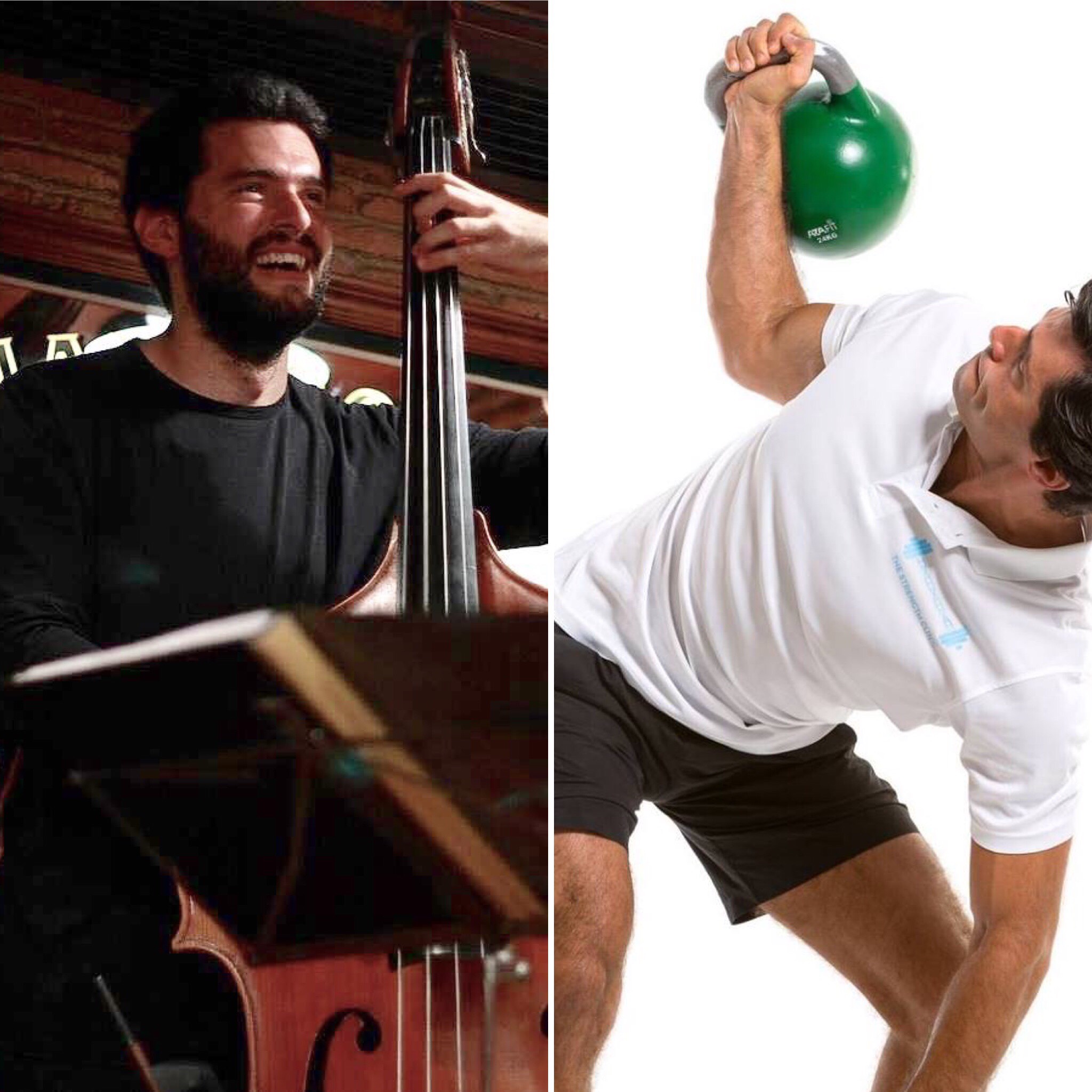
This is an article on a topic that is very special to me. I’m going to talk about myself, about music, about musicians, about sports and about physical preparation.
I will explain how it is possible to play at the highest level for many, many years in a healthy way and without having to practice endless hours of scales with perfect technique. I will explain how it is possible to avoid tendinitis and other musculoskeletal injuries that typically affect musicians sooner or later, which result from long hours of practice of repetitive gestures in very “unnatural” positions. Yes, it is possible to avoid, mitigate or even eliminate pain in your back, shoulders, neck, elbows, wrists and fingers, which are so common among professional musicians.
Me and music …
Those who have known me for less than 10 years probably don’t know, but I have had a career as a professional musician for at least the previous 10 years. I’ve started playing bass guitar and at a certain point I switched to double bass. I’ve studied at several schools in Portugal (Lisbon Conservatory, Lisbon Superior School of Music and Hot Club of Portugal Jazz School where I would become a teacher) and graduated from the Conservatory of Amsterdam. I was in fact obsessed with playing double bass and particularly obsessed with playing it with perfect technique! I used to practice a reasonable number of hours a day and was able to subject myself to incredibly boring exercises for many hours in a row, just because I wanted to improve a certain aspect of my performance. I could practice about 10 hours a day. For the less familiar with music instruments, the double bass is a very physically demanding instrument, and 10 hours of repetitive gestures in unbalanced positions is very stressful on the body.
Due to long hours of musical practice, I developed a debilitating neuromuscular pathology (focal dystonia) that led me to a long rehabilitation process and to put my music career on hold. To know what focal dystonia is follow this LINK. In addition to focal dystonia, the list of complaints included:
- Frequent back pain, particularly in the lower back;
- Pain and stiffness in the neck, the sensation of having a wry neck that never went away;
- A thoracic kyphosis already up to a non-physiological degree;
- Protruded (forward) shoulders;
- Uneven hips. Because I spent many hours standing leaning mostly over my right leg and in slight lateral flexion, my pelvis was tilted to that side, just like my torso and shoulder. In fact, my right side was all “shortened”, as if I had one leg shorter than the other, which anatomically does not occur;
- Highly rigid and weak wrists, hands and fingers. For instance, I could not hold a push-up position on the floor with arms straight and shoulders over the hands, because my wrists would hurt and did not extend enough.
To aggravate all these imbalances caused by specific and repetitive gestures, my choices for physical activity (yes, because my past in sports impelled me not to be sedentary) relied on activities that were also specific and that also included repetitive gestures, that is, I would play sports! By definition, any sport and its related gestures are specific, cyclic, repetitive and asymmetric. There are sports “less bad” than others, but they are all asymmetrical. And no, swimming is not a complete sport, none is!
All this, and particularly the highly traumatizing and time-consuming process of neuromotor retuning that I underwent to treat dystonia, has prompted me to better understand processes related to the neuromuscular function, motor control, and musculoskeletal injuries. I decided to go back to the university and start a new career, and discovered other obsessions: anatomy, physiology, nutrition, strength training. And here I am today!
Musicians and the myths about “frailty” of their fingers and body …
I have to acknowledge, and my musician friends must forgive me, but musicians are usually very lazy to do any physical activity. We live to play our instruments and to be available for rehearsals. We make up excuses such as not having time and / or that our working tools (e.g. hands and fingers) are very “sensitive” and prone to injury if we engage in any vigorous physical activity. The fear of twisting a finger or cutting a lip (for wind instrumentalists) or even a foot (for drummers) is understandable! In fact, a finger injury for example may be enough to impede a musician from working for several weeks.
Who hasn’t witnessed or lived the situation where when playing soccer with friends those who are musicians try to avoid playing as the goal keeper with fear of injuring their fingers? Perfectly legitimate and understandable. And it’s precisely for this reason that if musicians want to get in better shape and ensure they can play music without injuries for many more years, doing sports is not the solution. They can do it for pleasure, and the energy expenditure that results from it can have positive metabolic effects. However, all asymmetries and musculoskeletal injuries that result from playing an instrument will not be corrected by playing a particular sport and will most likely will be worsened.
Musicians should do general physical preparation instead! Because a professional musician is a highly specialized high-level athlete. A high-level athlete practices his sport and in his training program is (or at least should be) included a very important component which is basic physical preparation. In his physical preparation program our athlete trains for strength, mobility and endurance, and other physical qualities in order to establish a general athletic base that will make him more resilient and protect him from injuries that his sport, which is repetitive and asymmetrical, makes him vulnerable to.
We don’t get fit FROM PLAYING sports, we should get fit TO PLAY sports. The repetition of specific sports gestures induces specific musculoskeletal adaptations. It is easy to understand that for an athlete, it does not make sense to try to compensate for a specific adaptation induced by a sport gesture with another one which might apparently look as an opposite one! For example, will it be smart for a right-handed tennis player to try compensating for the asymmetries resulting from playing with his right arm by engaging in the practice of table tennis with his left arm? Or, if our player exhibits pain in the right shoulder associated with lack of flexibility and strength, does it make sense to start practicing gymnastics just because apparently gymnasts have strong and flexible shoulders? No and no! This athlete should follow a program of general physical preparation to become stronger and more mobile, which can in fact compensate for the asymmetries induced by the sport that he practices.
What is the similarity between playing an instrument and practicing a sport? It’s the same…
Imagine compensating for the unbalanced position of playing double bass with playing another instrument in a seemingly opposite position?
Let’s explore that idea…
For example, playing double bass (a string instrument that can be played with a bow or fingers of the dominant upper limb) implies (usually) standing in a position characterized by unilateral rotation and flexion of the torso, accompanied by a forward leaning of the trunk, in a bipedal position with greater weight over the side of the torso’s lateral flexion, with elevation of both non-dominant arm and shoulder paired with depression of both dominant arm and shoulder, and rotation and slight lateral flexion of the head.
So, to compensate for or correct all these adaptations will it make any sense to go play the violin for example? Because apparently, it’s the opposite! You are (usually) sitting and not standing, the rotation and flexion of the head is in the opposite direction, where both dominant arm and shoulder are apparently more depressed, and the dominant arm raised …? Of course not…
By the same token, this musician will not be stronger, more flexible and more resilient to injuries due to his musical practice if he chooses to compensate for these adaptations with the practice of a sport. If you enjoy playing football or tennis with friends, you should do so, but it will not make you more resilient to injuries or attenuate the ones you may already have.
You must go to the basics: physical preparation.
Musicians should follow physical preparation program such as an athlete. Playing an instrument is highly specific and doing it regularly and long-term will require some specificity and in terms of exercises that can compensate for those unnatural positions that are held for such long periods of time. Yet, the basis of physical preparation will always be (for the athlete, musician, or any other) of a general nature. It is necessary to make the body stronger and more flexible, because only that way one can make it more resilient in order to endure the highly demanding physical requirements of playing a musical instrument for hours, days and years on end.
The pain and discomfort that you my fellow musician feel now, can improve with physical training! Smart training in a controlled environment. A kind of training that can make all the structures of our body stronger and less rigid. A kind of training that promotes a better alignment of the kinetic chain and that enables you to produce force in fundamental movement patterns such as pulling, pushing, lifting objects off the floor, squatting, crawling, walking and jumping.
And no, your body is not fragile! If it hurts, it’s because it’s somehow weak!
Believe me, I’ve been there, done that… ?
Nos artigos anteriores desta série (ver aqui Parte 1 e Parte 2) discutimos o fato de que enquanto todos os golfistas vão fazer todos os possíveis para alterar o seu jogo (comprando tacos novos e bolas novas), muitos negligenciam um dos fatores mais decisivos para o seu sucesso físico e mental – a sua nutrição; identificamos algumas das principais razões pelas quais os golfistas nunca mudam e, finalmente, indicamos cinco ligações importantes entre o golfe e uma alimentação adequada. Neste artigo vou partilhar consigo as minhas preocupações sobre a dieta normal e os cinco hábitos mais importantes que deve criar para começar a nutrir melhor o seu corpo.
A Dieta Ocidental
A dieta ocidental é geralmente utilizada para descrever os hábitos alimentares popularizados nos EUA. Como esses hábitos alimentares são ainda muito populares na Europa e outras partes do mundo não-ocidental, provavelmente será necessário encontrar um novo nome para este tipo de “alimentação” nos próximos anos (talvez a dieta assassina seja um bom nome!).
Mas o que é a “dieta ocidental?” Bem, esta “dieta” pode ser resumidamente caraterizada por uma ingestão elevada de alimentos processados, hidratos de carbono refinados, açúcar e de gorduras hidrogenadas; e por uma baixa ingestão de frutas, verduras e gorduras saudáveis. É esta “dieta ocidental” que tem sido associada à maioria das doenças ocidentais ou doenças da civilização (exemplos: doenças cardiovasculares, obesidade, diabetes, cancro, alzheimer, parkinson). Curiosamente, esta dieta também pode ser a responsável pelo aumento da violência e pela diminuição dos resultados dos testes cognitivos nas crianças em idade escolar (défice de atenção) e nos adultos. Finalmente, esta “dieta ocidental” também tem sido associada à perda de massa óssea (osteoporose) e à diminuição de massa muscular (sarcopenia) em indivíduos adultos.
Vamos ver um exemplo de um menu diário de um “atleta normal” antes de trabalhar comigo.
Pequeno Almoço: Taça de cereais com leite + sumo de laranja natural + café com açúcar
Snack 1: Tosta mista + leite achocolatado
Almoço: Salada de frango com molho de maionese e ketchup + refrigerante + gelado
Snack 2: Fatia de bolo + sumo
Jantar: Peixe grelhado com verduras + batatas assadas + copo de vinho tinto + sobremesa
Para a maior parte das pessoas, isto até pode ser considerado um dia bom (e, de fato, há algumas coisas boas neste menu) mas no longo prazo este tipo de alimentação vai comprometer e muito a sua saúde e performance. Por este motivo há que discutir esta situação com a pessoa e atender às suas reais necessidades fisiológicas e funcionais.
Os Hábitos que deve criar
Antes de proceder à alteração da dieta, para mim o mais importante é que as pessoas comecem com uma base firme e sólida para, depois, efetuarem as mudanças necessárias para a otmização da sua saúde e performance. A maior parte das pessoas (atletas incluídos) quer começar a construir uma casa pelo telhado ou pelas paredes sem atender à qualidade do solo. Qualquer um destes hábitos são bastante simples, mas tal como qualquer hábito que pretenda criar, é preciso tempo de prática para assimilar as bases de uma nutrição correta.
Hábito 1 – Beber mais água
Por vezes falamos de tanta coisa no que diz respeito à alimentação e esquecemo-nos da água, o elemento mais importante que o nosso corpo precisa para funcionar corretamente. É a água que regula todas as funções do nosso corpo, incluindo a atividade de todos os solutos (os materiais sólidos) dissolvidos na mesma, ou seja, é a água, em primeiro lugar, que vai permitir que os nutrientes que consumimos cheguem às nossas células e aos nossos orgãos. Aponte para consumir 1-2 copos de água após acordar e para beber cerca de 2 litros/dia.
Hábito 2 – Comer uma fonte de proteína em todas as refeições
É fundamental comer proteína em cada refeição. Claro, alguns “especialistas” vão fazê-lo(a) acreditar no contrário, sugerindo que a proteína é de alguma forma prejudicial aos rins, desnecessária, etc. No entanto, eu quero destacar o fato que aquilo que procuro para os meus clientes/atletas é o melhor destes três mundos: melhor saúde, melhor corpo e melhor performance – será muito difícil alcançar estes três com uma ingestão sub-ótima de proteína. Alguns exemplos incluem: ovos, carne, peixe, frango, peru e marisco.
Hábito 3 – Comer verduras em todas as refeições
Os seus pais e/ou avós têm razão – você precisa de comer verduras para prevenir doenças! A evidência tem demonstrado que, para além dos micronutrientes (vitaminas e minerais) presentes nas verduras, há também fitoquímicos que são essenciais para o nosso funcionamento fisiológico ideal. As verduras vão ajudar a melhorar o equilíbrio ácido-base no corpo por isso o meu conselho todas as verduras que puder!
Hábito 4 – Comer uma fonte de gordura saudável em cada refeição
A gordura (tal como a proteína) é um macronutriente essencial e por esse motivo temos que garantir um aporte adequado todos os dias através da nossa dieta. Tem havido muita confusão em relação aos efeitos da gordura na dieta mas a verdade é que a gordura pode ser a nossa melhor amiga quando o objetivo é perder massa gorda, otimizar a resposta fisiológica do nosso corpo e a nossa saúde. Alguns exemplos de gordura saudável incluem: peixe gordo, oleaginosas, azeite virgem extra, côco e pêra abacate.
Hábito 5 – Comer mais verduras com as refeições principais e deixar os outros hidratos de carbono para a janela pós-treino
Outra forma de dizer isto é: se você tem gordura para perder, você tem que ganhar o direito a comer hidratos de carbono, fazendo exercício físico vigoroso em primeiro lugar! Quer continuar a comer pão, massa, arroz, batata, bolachas, alimentos açucarados, pizzas, doces, etc.? Você até pode comê-los – apenas tenha a certeza que o faz na janela pós treino (1-2 horas após o treino) porque esta é a altura que o seu corpo está mais sensível à insulina. Quanto à qualidade dos hidratos de carbono, terá mais benefícios se optar por alimentos sem glúten (arroz, quinoa, castanhas, batata-doce, inhame, batata) que pelos alimentos excessivamente processados e/ou com glúten – não aproveite o fato de fazer exercício para tratar o seu corpo como se fosse o camião do lixo!
Votos de um Bom Natal e Feliz Ano Novo!
Pedro Correia

Este é um artigo sobre um tema que me é muito caro. Vou falar sobre mim, sobre música, sobre músicos, sobre desporto e preparação física.
Vou explicar como é que é possível tocar ao mais alto nível durante muitos e longos anos de forma saudável e que não passa por praticar mais horas de escalas com técnica perfeita. Vou explicar como é possível evitar tendinites e outras lesões músculo-esqueléticas que mais cedo ou mais tarde acabam por afetar os músicos e que resultam das longas horas de prática de gestos repetitivos em posições muito pouco “naturais”. Sim, é possível evitar, atenuar ou mesmo eliminar as dores nas costas, ombros, pescoço, cotovelos, pulsos e dedos tão comuns entre músicos profissionais.
Eu e a música…
Os que me conhecem há menos de 10 anos provavelmente não sabem, mas tive uma carreira como músico profissional durante pelo menos os 10 anos anteriores. Comecei por tocar baixo elétrico e a dada altura transitei para o contrabaixo. Estudei em várias escolas em Portugal (Conservatório de Lisboa, Escola Superior de Música de Lisboa e Escola de Jazz do Hot Clube de Portugal onde viria a ser professor) e licenciei-me no Conservatório de Amesterdão. Eu era de facto obcecado por tocar contrabaixo e particularmente obcecado por tocá-lo com técnica perfeita! Estudava um razoável número de horas por dia e era capaz de me submeter a praticar exercícios incrivelmente chatos durante horas a fio porque queria melhorar um determinado aspeto da minha execução. Poderia praticar cerca de 10 horas num dia. Para os menos identificados, o contrabaixo em particular é um instrumento muito exigente em termos físicos, e 10 horas de gestos repetitivos em posições desequilibradas é muito desgastante.
Devido a longas horas de prática musical, desenvolvi uma patologia neuromuscular debilitante (distonia focal) que me levou a um longo processo de reabilitação e a suspender a minha carreira musical. Para saber o que é distonia focal sigam este LINK. Além da distonia focal, a lista de queixas incluía:
- Dores nas costas frequentes, sobretudo zona lombar;
- Dores e rigidez no pescoço, a sensação de ter um torcicolo que nunca passava;
- Uma cifose torácica já com algum grau não fisiológico;
- Ombros anteriorizados;
- Anca desalinhada. Como permanecia horas a fio em pé sobretudo apoiado sobre a perna direita e em ligeira flexão lateral, a minha bacia estava inclinada para esse lado, tal como o meu tronco e ombro. Na verdade, o meu lado direito estava todo “encurtado”, como se tivesse uma perna mais curta que a outra, coisa que anatomicamente não se verifica;
- Pulsos, mãos e dedos altamente rígidos e fracos. Não conseguia apoiar-me no chão numa posição para executar uma flexão por exemplo, porque os meus pulsos doíam e não faziam extensão suficiente.
Para agravar todas estes desequilíbrios provocados por gestos específicos e repetitivos, a minha opção de atividade física (sim, porque o meu passado como desportista impelia-me a não ser sedentário) recaia sobre atividades também elas específicas e que incluíam gestos repetitivos, ou seja, a prática de desportos! Por definição, um gesto ou prática desportiva é específica, cíclica, repetitiva e assimétrica. Há desportos mais generosos que outros, mas são todos assimétricos. E, não, a natação não é um desporto completo, nenhum é!
Tudo isto, e particularmente o processo (altamente traumatizante e moroso) de reprogramação neuro-motora para tratar a distonia impeliu-me a querer entender melhor processos relacionados com a função neuromuscular, controlo motor e lesões músculo-esqueléticas. Decidi voltar para a faculdade e encetar uma nova carreira e descobri outras obsessões: anatomia, fisiologia, nutrição, treino de força. E aqui estou hoje!
Os músicos e os mitos sobre a “fragilidade” dos seus dedos e corpo…
Tenho que reconhecer, e perdoem-me camaradas músicos, mas a malta é em geral preguiçosa para fazer atividade física. Vivemos para tocar os nossos instrumentos e para estar disponível para ensaios. Desculpamo-nos com falta de tempo e/ou com o argumento de que o nosso instrumento de trabalho (e.g., mãos e dedos) serem muito “sensíveis’’ e passíveis de se lesionarem em atividades mais vigorosas. O medo de torcer um dedo ou cortar um lábio (nos casos dos instrumentistas de sopro) ou mesmo um pé (no caso dos bateristas) é legitimo! De facto, lesionar-se num dedo por exemplo pode ser o suficiente para não poder trabalhar durante várias semanas.
Quantos de nós é que já não estiveram na situação de estar a jogar futebol com os amigos e aqueles que são músicos tentarem esquivar-se de jogar na baliza para não se lesionarem nos dedos? Perfeitamente legítimo e compreensível. E é precisamente por isto que se os músicos pretenderem ficar em melhor forma física e garantir que podem tocar sem lesões durante muito mais anos, fazer desporto não é a solução. Podem fazê-lo por prazer, e o dispêndio energético poderá ter efeitos metabólicos positivos. Contudo, todas as assimetrias e lesões músculo-esqueléticas que decorrem de tocar um instrumento não são colmatadas e muito provavelmente são acentuadas.
Os músicos devem sim privilegiar fazer preparação física geral! Porque um músico profissional é um atleta de alta competição altamente especializado. Um atleta de alta competição pratica o seu desporto e no seu programa está incluída uma componente importantíssima de preparação física de base. Aí o nosso atleta treina força, mobilidade e resistência e outras qualidades físicas no intuito de estabelecer uma base atlética geral que o torne mais resiliente e o proteja das lesões que o seu desporto, que é repetitivo e assimétrico, induz.
Não se fica em forma POR fazer desporto, preparamo-nos fisicamente PARA fazer desporto. A prática de gestos desportivos, específicos e repetidamente induz adaptações músculo-esqueléticas específicas. Será fácil de entender que este nosso atleta não faz sentido compensar uma adaptação induzida por um gesto desportivo específico com outro aparentemente oposto. Por exemplo, não será inteligente para um jogador de ténis destro compensar as assimetrias decorrentes de jogar com o braço direito com a prática de ténis de mesa com o braço esquerdo? Ou, se o nosso jogador exibir dor no ombro direito associada a falta de flexibilidade e força, não faz sentido iniciar-se na prática de ginástica desportiva porque, aparentemente os ginastas têm ombros fortes e flexíveis? Este nosso atleta tem que seguir um programa de preparação física geral para ficar mais forte, flexível e que compense as assimetrias induzidas pelo desporto que pratica.
Qual a semelhança entre tocar um instrumento e praticar um desporto? É igual…
Imaginem compensar a posição desequilibrada de tocar contrabaixo com tocar outro instrumento com uma posição aparentemente oposta?
Senão vejamos…
Tocar contrabaixo de cordas (instrumento de corda que pode ser friccionada ou dedilhada) implica a permanência numa posição em pé com rotação e flexão unilateral, acompanhada duma inclinação do tronco, numa posição bipedal com maior peso sobre o apoio do lado da flexão lateral, e ainda com elevação do braço e ombro não dominantes e depressão dos dominantes e rotação e ligeira flexão lateral da cabeça.
Então, para compensar todas estas adaptações fará sentido ir tocar violino por exemplo? Porque aparentemente é oposto! É sentado e não em pé, a rotação e flexão da cabeça é no sentido oposto, e o braço e ombro dominante estão aparentemente mais deprimidos e o braço dominante elevado…? Claro que não…
E na mesma lógica, este nosso músico também não ficará mais forte, flexível e resistente a lesões decorrentes da sua prática musical se escolher tentar compensar essas adaptações com a prática de um desporto. Se gosta de jogar futebol ou ténis com os amigos, deve fazê-lo, mas isso não o tornará mais resiliente e não atenuará lesões que possa já exibir.
Há que ir ao básico: preparação física.
Os músicos deverão fazer preparação física tal como um atleta. A sua atividade altamente específica e executada durante longos períodos irá requerer alguma especificidade e em termos de exercícios que compensem as posições não naturais que são mantidas durante muito tempo, contudo a base dessa preparação física será sempre (para o atleta, músico ou qualquer outro) de carácter geral. Há que tornar o corpo mais forte e flexível, por que só assim resistirá melhor à exigência física que é tocar um instrumento musical durante horas, dias e anos a fio.
As dores e desconforto que os meus amigos músicos sentem agora podem melhorar com treino! Treino inteligente e num ambiente controlado. Treino que torne todas as estruturas do nosso corpo mais fortes e menos rígidas. Treino que promova melhor alinhamento da cadeia cinética e capacidade de produção de força em padrões de movimento fundamentais, tais como: puxar, empurrar, levantar objetos do chão, agachar, gatinhar, caminhar e saltar.
E não, o vosso corpo não é frágil! Se ele dói, é porque está fraco!
Acreditem, eu já estive aí… ?
Nuno Correia

O pé e o tornozelo constituem a base de sustentação do corpo humano proporcionando a estabilidade necessária para assumir uma postura bípede. O comprometimento da mobilidade do tornozelo causada por adaptações posturais às atividades diárias e uso de calçado inadequado (particularmente saltos altos) poderá ter implicações na execução de gestos característicos à maioria das modalidades desportivas, assim como em muitos exercícios presentes em programas de treino de força.
Como é que restrições na dorsiflexão do tornozelo podem causar limitações funcionais comprometendo o rendimento desportivo e constituir um fator de risco de lesão?
– Uma dorsiflexão limitada pode causar alterações na cinemática no plano sagital (diminuição da flexão e excursão) e frontal (aumento do valgo dinâmico) da articulação do joelho durante a realização de exercícios como o Agachamento. A restrição no plano sagital resulta também em alterações nos padrões de ativação muscular do solear (aumento) e quadríceps (diminuição) durante a fase excêntrica do Agachamento (Macrum et al., 2012). Estas condicionantes podem tornar um indivíduo mais suscetível ao uso excessivo ou de lesões agudas do joelho, como a síndrome patelo-femoral.
– A lesão do ligamento cruzado anterior (LCA) ocorre normalmente durante a participação em atividades desportivas através de um mecanismo sem contacto envolvendo uma mudança súbita de direção, paragem repentina, receção ao solo após um salto (ou combinação de ambas). Restrição na dorsiflexão durante a receção ao solo está associada a uma menor flexão do joelho, maiores forças de reação do solo e consequentemente a um aumento do valgo dinâmico (Fong et al., 2011). Estes fatores biomecânicos estão inter-relacionados, resultando num risco acrescido de lesão do LCA.
– O Single Leg Squat Test (SLST) é comumente utilizado para avaliar o valgo dinâmico e consequentemente o potencial risco de lesão ao nível do membro inferior, assim como o retorno à atividade desportiva irrestrita após a reconstrução do LCA. Está correlacionado com tarefas como receção ao solo após um salto, corrida e mudanças de direção. Num estudo (Mauntel et al., 2013) onde se correlaciona o desvio medial do joelho durante o SLST com a ativação muscular e amplitude de movimento articular passiva do membro inferior, a restrição na dorsiflexão foi um dos aspetos relacionados com o desvio medial do joelho.
Dessa forma os programas de treino de força e condição física, reabilitação e prevenção de lesões devem ter em conta possíveis restrições na dorsiflexão do tornozelo com vista à diminuição da incidência de lesões no membro inferior.
Patrick Filipe
Referências:
Macrum, E. Bell, D. Boling, M. Lewek, M. Padua, D. 2012. Effect of Limiting Ankle-Dorsiflexion Range of Motion on Lower Extremity Kinematics and Muscle-Activation Patterns During a Squat. Journal of Sport Rehabilitation, 21, 144-150.
Fong CM, Blackburn JT, Norcross MF, McGrath M, Padua DA. 2011. Ankle-dorsiflexion range of motion and landing biomechanics. Journal of Athletic Training. 46(1):5–10.
Mauntel TC, Begalle RL, Cram TR, Frank BS, Hirth CJ, Blackburn T, Padua DA. 2013. The effects of lower extremity muscle activation and passive range of motion on single leg squat performance. Journal of Strength and Conditioning Research 27(7)/1813–1823.
Você já se perguntou porquê que a maioria das pessoas come de forma muito parecida? Um pequeno almoço com leite e cereais, uma sopa e uma sandes à hora de almoço e, com sorte, um jantar um pouco mais equilibrado com carne ou peixe, arroz e algumas verduras? E aqueles snacks a meio da manhã e/ou tarde de café com torradas? De bolachas? De bolos com refrigerantes? De barras de cereais? Você acha que isto é coincidência? Claro que não, isto não acontece por acaso!
Isto só acontece desta forma porque foi assim que você foi ensinado a comer. Talvez seja esta a maneira que os seus pais comem. Talvez seja esta a maneira como a sua esposa, marido ou companheiro(a) come. Talvez seja esta a maneira que os seus amigos e/ou colegas de trabalho comem. Talvez seja esta a maneira que os seus companheiros de equipa comem. Na verdade, as pessoas nem se apercebem se aquilo que estão a comer é adequado ou não para a nossa fisiologia e genética, se melhora ou piora a saúde, se melhora ou piora a performance, elas comem desta maneira porque este é o padrão alimentar que seguem há muitos anos, e estes foram os hábitos que criaram.
No último artigo abordamos várias razões pelas quais os golfistas negligenciam a nutrição, um dos aspectos que mais podem influenciar a sua performance no campo de golfe. É curioso verificar que a maioria dos golfistas está mais preocupada com os tacos topo de gama e com os novos acessórios que aparecem do que com os alimentos que comem. E é por este motivo que hoje vou apresentar cinco razões para você melhorar a sua alimentação.
Pense um bocadinho nisto. Se você soubesse que comer e/ou suplementar de uma determinada forma iria: 1) reduzir a sua massa gorda; 2) aumentar a sua força muscular; 3) melhorar a sua saúde óssea; 4) permitir uma recuperação mais rápida; 5) aumentar a sua distância do tee; 6) melhorar o seu humor; 7) reduzir as sensações de ansiedade e raiva; 8) melhorar a sua concentração e criatividade; 9) melhorar virtualmente qualquer marcador de saúde conhecido e 10) melhorar a sua performance nas sessões de treino e/ou na competição, você estaria disposto a comer dessa forma? Tendo em conta esta pequena lista de beneficios acho que valeria a pena experimentar. Fique comigo.
- Comer bem vai melhorar a sua composição corporal
O seu peso corporal total é a soma da sua massa magra e da sua massa gorda. A massa magra é constituída pela massa muscular, orgãos, ossos, sangue e pele. A sua massa gorda é basicamente toda a gordura que tem acumulada no corpo. Para um indivíduo ser considerado atlético, este precisa de manter uma boa relação entra a massa magra e a massa gorda. E os golfistas não devem ser excepção. Com isto eu não pretendo dizer que todos os golfistas precisam de ter os abdominais do Cristiano Ronaldo, aquilo que pretendo dizer é que, em circunstâncias normais, o excesso de gordura corporal não tem quaisquer benefícios (a não ser que você seja lutador de sumo nas horas vagas). Um excesso de gordura corporal vai afectar a eficiência do seu swing, a sua mobilidade e a sua potência rotacional, ou seja, você vai ter maiores dificuldades em mover o corpo quando transporta gordura em excesso. Quanto mais massa gorda tiver, mais força terá que usar para mover o corpo – a gordura vai “roubar” potência ao seu swing. Portanto, não é o tecido adiposo que vai imprimir potência à sua pancada, é o seu tecido muscular!
- Comer bem vai melhorar a recuperação
Se você está seriamente comprometido em melhorar o seu jogo, você sabe que é preciso praticar (e muito!). Segundo os especialistas, alguns golfistas profissionais podem chegar a bater 600 bolas por dia incluindo chips e putts. E para realizar todos estes swings é preciso ter força e potência muscular, ou seja, é preciso fazer algum tipo de trabalho no ginásio! Se o corpo não estiver preparado para lidar com este tipo de stress de forma crónica, as lesões e as dores vão começar a aparecer. Se você costuma acabar as suas sessões de treino de golfe dorido, se nota oscilações na motivação, se já não consegue bater bolas de forma coordenada, se nota reduções no apetite e se fica acordado à noite apesar de estar a treinar bastante, é muito provável que a sua recuperação não esteja a ser a melhor. Os danos musculares, a fadiga do Sistema Nervoso Central e o over-reaching são sintomas bastante característicos de muitas modalidades mas os golfistas têm tendência a não olhar para estas coisas. Apesar do golfe não ser tão fisicamente exigente como outras modalidades, a verdade é que o volume de treino diário a que o corpo é sujeito é grande e isso vai fazer com que a nutrição seja uma peça fundamental na recuperação.
- Comer bem vai melhorar o humor, a concentração e o foco
Qualquer golfista profissional no PGA Tour e/ou no European Tour é capaz de vencer qualquer grande evento. Mas porquê que alguns se destacam de forma mais consistente do que outros? Porque, segundo os especialistas, aqueles que se destacam são mentalmente inabaláveis. Ou seja, a sua capacidade de desligar o diálogo interno negativo, de relaxar o cérebro de forma consciente e de manter o foco com uma concentração imperturbável é impressionante. Alguns consideram que isto é uma habilidade inata. E é, de facto. Mas pode ser treinada! Contudo, há também uma base bioquímica para estas proezas mentais. Você deve saber que, ao fornecer os nutrientes corretos, incluindo suplementos nutricionais, nos momentos certos, a ligação fisiológica entre o cérebro e os músculos pode ser reforçada. Tal como o foco e a concentração. Por exemplo, ao controlar os seus níveis de glicémia no sangue com refeições frequentes e menos açúcar na dieta, as flutuações de humor e aquela sensação de pouca energia após o almoço podem ser eliminadas. Portanto, além da composição corporal e recuperação, a nutrição pode afectar fortemente o seu jogo mental. Com os nutrientes adequados, a concentração, a eficiência neuromuscular e o humor podem ser melhorados de forma significativa. Pelo contrário, se você não ingerir estes nutrientes, a fadiga vai aparecer mais cedo e você já não vai ser capaz de se concentrar da mesma forma.
- Comer bem vai melhorar a sua saúde
Quando estou a falar de saúde não me refiro apenas à ausência de dor e/ou doença, refiro-me a uma sensação de bem estar físico, emocional e mental. Para render ao mais alto nível é preciso que a saúde seja optimizada e por esse motivo a definição de saúde que eu partilho com os meus clientes / atletas engloba: 1) um sistema imunitário resiliente; 2) sistemas antioxidantes fortes que protejam contra radicais livres; 3) bons sistemas de desintoxicação; 4) um bom equilíbrio de bactérias no intestino; 5) um equilíbrio de alimentos básicos e ácidos; 6) baixos níveis de inflamação no corpo; 7) um equilíbrio ideal entre massa gorda e massa magra; 8) um bom equilíbrio de ácidos gordos; 9) uma boa sensibilidade à insulina; 10) altos níveis de energia e 11) a capacidade de maximizar a performance mental e física em qualquer idade. Todos estes marcadores de saúde podem ser influenciados pelos alimentos que comemos todos os dias! Portanto, estas estratégias nutricionais não vão apenas ajudá-lo a prevenir doenças como também a optimizar a sua função corporal e a render ao mais alto nível.
- Comer bem vai melhorar o seu rendimento nos treinos e competição
Para a maior parte de vocês não é nenhuma surpresa constatar que a maioria da nutrição no campo de golfe é pobre, variando de sandes mistas e cerveja para bebidas desportivas e “barras energéticas” (nota: a maioria dos quais são basicamente barras de chocolate cheias de açúcar e de gordura de má qualidade) com um rótulo aparentemente saudável. Este tipo de alimentos não estão certamente a prepará-lo para performances dignas de registo, aliás, eu diria mesmo que estes alimentos até vão prejudicar a performance. Por exemplo, a cerveja, é um depressor do sistema nervoso central, reduzindo a concentração e o controle motor. As bebidas desportivas (ex: Powerade), as sandes (mesmo as integrais!) e as “barras energéticas” vão elevar abruptamente os níveis de açúcar no sangue, ou seja, aquilo que aparentemente é bom porque leva a uma subida de energia rápida acaba por ser mau porque depois vamos assistir a uma quebra de energia cerca de 45/60 minutos depois. Quando os níveis de açúcar no sangue caem a pico, o humor piora, o foco e a concentração diminuem – e, claro, a performance, piora!
Para optimizar a sua performance no treino e na competição, há pelo menos três coisas que são necessárias. Primeiro, você deve manter uma boa hidratação, especialmente em climas quentes e húmidos. Mesmo uma pequena desidratação pode reduzir a coordenação e o controle motor. Em segundo lugar, você deve controlar os níveis de açúcar no sangue. Isto não significa que você deve comer alimentos ricos em açúcar mas sim alimentos que ajudem a manter os níveis de glicémia estáveis. Em terceiro lugar, você deve recorrer a algumas estratégias nutricionais e/ou suplementos que lhe ajudem a aumentar o foco e a concentração. Resumindo, não continue a depender daquilo que lhe oferecem nos carrinhos-bar dos campos de golfe – provavelmente a única coisa saudável que eles lá têm é água!
Bons treinos!
Pedro Correia
Todos os jogadores de golfe têm uma característica em comum: eles vão investir bastante tempo e dinheiro para melhorar o seu jogo! Eles vão contratar os melhores treinadores para aperfeiçoar o seu swing de golfe. Eles vão comprar o melhor equipamento disponível para obter mais precisão e ganhar distância. Aqueles que já perceberam a importância da preparação física nesta modalidade vão contratar os melhores profissionais para ajudá-los a ganhar mobilidade, a ficar mais fortes e com maior resistência física. Alguns vão recorrer aos psicólogos desportivos para aprender como manter uma boa atitude em campo, o foco e a concentração. Eles fazem tudo isto com o objetivo de fazer mais birdies. Mas será que eles não se estão a esquecer de nada?
No meio de tudo isto há algo que a maioria dos golfistas se esquece de alterar: a sua dieta de baixa qualidade. A maioria dos golfistas não faz a mínima ideia de como é que a dieta pode influenciar a performance. Para começar, eles esquecem-se que comer mal vai comprometer o aumento de força muscular e vai levar à acumulação de gordura corporal. E se você ainda pensa que ter músculos fracos e excesso de gordura corporal é o caminho a seguir para tornar-se um golfista de alto nível, nem vale a pena continuar a ler. Este artigo não é para si.
Além dos efeitos na composição corporal e no défice de força muscular é preciso ter em conta que comer mal vai limitar o foco e concentração, vai levar a alterações de humor e pode levar a uma má função imunológica, a um aumento da inflamação crónica e a problemas de saúde em geral. Experimente jogar várias rondas durante dias seguidos quando está de mau humor, em má forma física, e não se consegue concentrar. Uma nutrição de má qualidade vai ter um impacto directo nos treinos e na competição. A falta de foco, de concentração e o cansaço precoce, especialmente durante os treinos e/ou competições, são sinais que a sua nutrição está a comprometer a sua performance.
Não tenha dúvidas: você até pode ser muito habilidoso com os tacos, fazer uns shots à Ballesteros e fazer umas rondas excepcionais de vez em quando, mas se aquilo que você procura é consistência nos resultados e longevidade enquanto golfista, não há nenhum substituto melhor que os alimentos que você come todos os dias. Nenhum!
Então porquê que os golfistas nunca mudam?
Existem várias razões pelas quais os golfistas nunca mudam e preferem continuar a comer as club sandwiches, as batatas fritas e os pratos de massa que existem em todos os clubhouses do Mundo. Vamos ver algumas.
1) O mito da refeição pré-competição.
Muitos golfistas (especialmente os principiantes) cometem o erro de pensar que são apenas os alimentos comidos antes e durante os treinos e jogos que podem afectar o seu jogo. Embora isto possa fazer sentido à primeira vista, não é isso que acontece do ponto de vista fisiológico – a maior parte da energia que você está a utilizar hoje depende dos nutrientes que comeu (e absorveu) nas últimas 72 horas!
Atenção, eu não estou a dizer que aquilo que você come antes e depois dos treinos/competições não faz diferença. É claro que faz! No entanto, essas refeições não são necessariamente as mais importantes. Cada refeição vai ter um determinado impacto no seu corpo independentemente do espaço temporal em que a mesma é consumida. É o efeito cumulativo dessas refeições que vão levar a uma melhoria (ou diminuição) da performance.
Por outras palavras, no golfe, não há nenhuma refeição mágica pré-competição ou intra-competição. Se você esperou até o dia antes de uma grande competição para começar a comer bem, é bem provável que já seja tarde demais. Lamento informar mas não há soluções milagrosas, você precisa mesmo de comer bem de forma consistente!
2) Os golfistas não conseguem ver a ligação entre a nutrição e a performance.
A maioria dos golfistas não percebe a lógica entre a nutrição e a performance. E isso acontece porque eles não estão conscientes de como é que a alimentação vai influenciar a sua função muscular e a bioquímica do cérebro.
No caso do golfe, como esta é uma modalidade que não envolve um dispêndio energético muito grande e que não obriga os atletas a manter um certo peso corporal (como acontece com os lutadores, ginastas, nadadores, atletas de endurance ou atletas de outros desportos), pensa-se que a necessidade de comer bem não é assim tão importante. Ou seja, não é assim tão óbvia essa relação.
Mas a questão fundamental não é essa, não é preciso que os golfistas sejam indivíduos musculados e com baixa percentagem de gordura corporal como você vê nas revistas de fitness. Aquilo que eles precisam é de desenvolver o seu potencial atlético para este não ser um factor que possa prejudicar a sua performance no campo de golfe. O golfe não é um desporto muito intenso do ponto de vista energético pelo que as necessidades nutricionais de um golfista não podem ser iguais às de um lutador ou de um atleta de endurance. Mas diferentes não significa menos importantes – como vimos acima não é apenas a composição corporal que vai ser influenciada pela alimentação.
Apesar da ligação entre o golfe e a nutrição ser um pouco menos visível que nos outros desportos, ela existe. A manutenção e/ou aumento da massa muscular, os ganhos de mobilidade, a redução da inflamação dos músculos e articulações, a manutenção do foco e concentração, a prevenção de lesões, todos estes aspectos podem ser influenciados pela nutrição. Mas só aqueles que colocarem as melhores estratégias nutricionais em prática é que terão vantagens competitivas (é óbvio que isto não inlcui Big Macs!).
3) A dificuldade em mudar os hábitos alimentares.
Provavelmente o obstáculo mais difícil para a maioria das pessoas é superar os hábitos alimentares que têm. Os nossos padrões alimentares já existem há muito tempo e são poucas as pessoas que estão dispostas a mudá-los se não houver uma razão muito forte para tal (como no caso de um problema grave de saúde). E porquê que isso acontece? Porque nós não fomos ensinados a pensar que os alimentos são informação para as nossas células. Nós não fomos ensinados a pensar que os alimentos vão influenciar a expressão dos nossos genes. Nós não fomos ensinados a pensar que são os alimentos que consumimos os gatilhos ambientais que vão contribuir para a melhoria da saúde ou para a sua deterioração.
É claro que existem muitas outras razões que explicam a relutância dos golfistas para mudar os seus hábitos alimentares e que explicam porquê que você não muda os seus. E é por esse motivo que no próximo artigo vou continuar a abordar este tema para você perceber porquê que precisa de mudar os seus hábitos alimentares rapidamente para viver com mais saúde e para poder levar o seu jogo para o próximo nível.
Bons treinos!
Pedro Correia

A Força de Preensão está correlacionada com a força dos membros superiores, força geral do corpo e capacidade funcional, assim como, estado nutricional, densidade mineral óssea, fatores de risco cardiovascular e mortalidade.
Como é que a Força de Preensão pode ter um papel importante na prevenção de lesões, reabilitação e desempenho desportivo?
– Padrões de co-ativação: Existe uma conexão neurológica entre a preensão manual e a coifa dos rotadores. Isso significa que o feedback propriocetivo dos nervos periféricos tem um impacto direto sobre a excitabilidade dos músculos da coifa dos rotadores, melhorando a centragem da cabeça do úmero e auxiliando na estabilização do ombro durante o uso do braço e mão.
– Irradiação: Quando um músculo contrai de forma intensa emite impulsos neurais que atingem os músculos adjacentes, fazendo com que estes participem na ação, aumentando a estabilidade postural e permitindo uma transferência de força mais eficiente.
– Dor no Cotovelo: Das inúmeras razões que podem levar a sintomas de dor ao nível do cotovelo, uma das causas pode ser a relação de forças inadequadas entre os músculos do cotovelo e músculos do antebraço. Se os flexores do cotovelo forem muito fortes em relação aos flexores do antebraço, a tensão irregular acumula-se nos tecidos moles provocando dor.
– Avaliação e Controlo da Performance: Sendo a força de preensão um excelente preditor da força total do corpo, este pode ser utilizado como elemento de avaliação e controlo da performance desportiva. Valores de força de preensão abaixo dos valores de referência (individuais) ou dos aferidos no início da sessão de treino anterior, pode ser um indicador de fadiga.
Quantas mais razões são necessárias para ter um bom “aperto de mão”?
Patrick Filipe
Referências:
National Conference & Exhibition Bridging The Gap 2016. Grip Strength: Unleash the secret to primal strength, injury prevention, and overall health. Dr. Arianne Missimer.

Para manterem a função física, recuperarem melhor de lesões, manterem massa magra e manterem-se mais saudáveis de um modo geral, indivíduos mais velhos necessitam de uma maior ingestão de proteína do que indivíduos jovens. Uma ingestão maior de proteína contribui para atenuar processos inflamatórios e catabólicos, bem como o decréscimo de eficiência no metabolismo da proteína associado com a idade.
De acordo com as recomendações avançadas pelo PROT-AGE Study Group (2013) (referência abaixo), indivíduos mais velhos deverão:
– ingerir PELO MENOS 1 a 1.2 g/kg de peso corporal de proteína por dia;
– ingerir AINDA MAIS se sofrem de doenças agudas ou crónicas, entre 1.2-1.5 g/kg de peso corporal de proteína por dia;
– ingerir AINDA MAIS se se encontram sub-nutridos e/ou sofrem duma doença ou lesão severa, ~2g/kg de peso corporal de proteína por dia;
– limitar a ingestão de proteína se sofrem de DOENÇA RENAL SEVERA E NÃO ESTÃO EM HEMODIÁLISE, sendo portanto UMA EXCEPÇÃO. E não, a doença renal NÃO é provocada pela ingestão de proteína;
– usar suplementação para atingir os níveis de ingestão de proteína desejados;
– E, claro, FAZER EXERCÍCIO que promova de forma mais eficaz a manutenção ou incremento de massa magra, ou seja, treino de força.
E não, a doença renal NÃO é causada pela ingestão de proteínas. Num estudo em que se acompanhou durante o período de um ano homens treinados em treino de força que consumiam ~2,51-3,32g/kg de peso corporal por dia durante um ano, não se verificou quaisquer efeitos prejudiciais no perfil lipídico de no sangue, bem como nas funções hepática e renal (Antonio et al, 2016).
A manutenção de força e massa magra (inclui massa muscular, massa óssea e do tecido conjuntivo) estão identificados como os primeiros e mais relevantes biomarcadores de saúde e longevidade. A melhoria destes marcadores produz um “efeito dominó” positivo e poderoso na grande parte (provavelmente todos) dos outros marcadores de saúde. A ingestão adequada de proteína e treino de força é essencial para construção de massa magra. E ainda mais determinante à medida que envelhecemos para contrapor a inevitável perda progressiva de eficiência no nosso metabolismo.
Não receie a proteína nem o treino de força. Estes são, provavelmente, dois dos seus melhores aliados para viver melhor e mais tempo.
Bom almoço e não se esqueça da proteína!
Nuno Correia
Referências:
Bauer, J. et al., 2013. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the prot-age study group. Journal of the American Medical Directors Association, 14(8), pp.542–559.
Antonio, J., Ellerbroek, A., Silver, T., Vargas, L., Tamayo, A., Buehn, R., & Peacock, C. A. (2016). A High Protein Diet Has No Harmful Effects: A One-Year Crossover Study in Resistance-Trained Males. Journal of nutrition and metabolism, 2016, 9104792.

Whatever the sport, strength training, in harmony with various training factors (i.e., technical, tactical, physical and psychological) and training principles (i.e., overload, specificity, reversibility, heterochronism, specialization, continuity, progression, cyclicity, individualization and multilateralism) will endow the athlete with a complete set of tools in order to maximize performance.
In tennis, strength is used to generate speed, power and endurance. It is impossible to have agility, speed, power, a developed anaerobic system, and flexibility / mobility without optimal strength levels (Verstegen, 2003). Strength training is also critical to prevent injury. Because tennis is a sport that involves many repetitions of movements of unilateral features, it is conducive to developing muscular imbalances which significantly increase the likelihood of injury. In tennis, the highest incidence of injuries is in the shoulders and back, followed by injuries in the elbows, knees and ankles (Kibler & Chandler, 1994). Thus, specific strength training for tennis is essential to maintain or restore proper muscle balance.
Definition of Force
The definition of force based on its purely mechanical concept consists of any cause capable of modifying the state of rest or motion of a body, consisting of a vector with a given magnitude and direction. It is the product of mass by acceleration (F=m*a). Although this definition of force is unanimously accepted, it hardly illustrates the different components of muscle strength. That is, if we understand muscle strength as an essential component for the development of motor skills which consists of the ability to apply force to overcome resistance (O’Sullivan & Schmitz, 1998).
Why Strength Training in Tennis?
A strength training program in the context of tennis should aim at developing “highly innervated muscles with an explosive ability” so that players can serve with greater speed, so that they can put “more weight” on the ball (due to an improved use of ground reaction forces), so that they can cover more area on court (because they are more agile and fast), and so that they feel as if they “float” on the court the whole day and week (Verstegen, 2003). It is important though to dispel some myths regarding strength training, namely that this type of training will make players slower, less agile or tight. Only poorly designed strength training programs will lead to this. In fact, several studies show that amongst Olympic athletes, weightlifters are those displaying the highest levels of power and are second best (after gymnasts) regarding flexibility levels (Jensen & Fisher, 1979).
It has been well established that adequate strength training not only maintains levels of flexibility but can actually significantly increase them (Fox, 1984; Jensen & Fisher, 1979; O’Shea, 1976; Rash, 1979). Also, adequate strength training induces significant improvements in: work capacity; body composition (i.e., lean mass gains and loss of fat mass); energy efficiency; tissue growth hormonal secretion profile favoring protein synthesis (e.g. strength training induces growth hormone secretion and testosterone); posture; and muscle balance (Lamb, 1984; Stone et al., 1982).
Specifically in tennis, it has been shown that strength training strengthens the immune system (thus protecting the player from injury and illness), and is often pointed to have a positive psychological effect on players, since it appears to be coupled with an increase in levels of self-confidence during matches (Folkins & Sime, 1981; Tucker, 1983), as out of the game (Folkins & Sime, 1981).
The Various Types of Strength and Its Application in Tennis
- Strength endurance: the ability to produce force over time while resisting to fatigue. Good strength endurance levels allow the maintenance of proper form and a correct technical execution. Together with the static strength, strength endurance makes a sort of a basis for developing other types of strength training in tennis.
- Static strength: the ability to stabilize joint structures allowing better transmission of energy along the kinetic chain, i.e. without loss of energy. In tennis, this type of strength allows optimal use of force generated against the ground to subsequently transfer speed to the ball.
- Maximal strength: relates to the maximal force value during a voluntary contraction against an immovable resistance. It is mainly a strength assessment parameter and we can consider its absolute and relative measures (i.e. relative to body weight). For tennis, relative strength is more relevant than absolute strength because it has a direct influence on the player’s speed and agility. Strength Deficit (SD) should also be evaluated based on measures for Maximum Eccentric Force (MEF) and Maximum Isometric Force (MIF). The SD = MEF-MIF. If the SD > 25% for the lower limbs, and SD > 50% for the upper limbs, training should prioritize Rate of Force Development (RFD). If below these values, strength training should focus on hypertrophic and maximal strength methods.
- Power – the ability to produce the most amount of force in the shortest time interval. It includes:
- Starting strength (up to 250ms of the force / time curve) –expressed as the Initial Force Production Rate (IFPR) and reveals the ability to accelerate from a static position (i.e., velocity = 0);
- Explosive force (above 250 ms of the force / time curve) – expressed as the Maximum Force Production Rate (MFPR) and reveals the ability to accelerate to maximum force levels. It is one of the main indicators of performance in tennis. It corresponds to the phase of maximum acceleration during a given movement;
- Reactive force – force produced during muscle’s stretch-shortening cycle (SSC). The use of the elastic and reflex properties of the muscle present in the SSC influences the IFPR and the MFPR. Reactive force training (i.e., using muscle’s SSC) may contribute to increased acceleration capacity, that is, increasing IFPR and the MFPR, and consequently gains in power.
- Optimal Strength (Verstegen, 2003): the combination of the types of strength described above according to aspects inherent to the player and his/her performance, such as: age; capacities; style of playing; stage of development; type of surface on which they will play.
Table 1 specifies the ideal characteristics of strength training in tennis for the various stages of development according to the Long-term Athletic Development model (Balyi & Hamilton, 1999).
| Table 1. | |||
| Age | Characteristics | ||
| 6-9 Boys 6-8 Girls | Strength training should focus on exercises with body weight. It may include the use of medicinal balls (of adequate weight) in exercises of a playful nature. The strength gains at this age are mainly attributed to gains in motor coordination and neuromuscular activation. | ||
| 9-12 Boys 8-11 Girls | Strength training should be regular and lead to progressive improvements. At this stage, however, emphasis should be placed on motor learning and development. | ||
|
12-16 Boys 11-15 Girls | Strength training should be characterized by short sessions (less than 30 minutes) two to three times a week. The Peak Height Velocity (PHV) will determine the increase in volume and intensity of the loads. Critical periods for strength training will occur shortly after PHV for girls, and 12-18 months after PVA for boys. Basic Olympic lifts techniques should be introduced and mastered during the PHV. This can constitute an important training tool “in the box” for later development high levels of power, as well as preventing injuries and optimize adaptation to strength training. | ||
| 16-18 Boys 15-17 Girls | Strength training should be regular and lead to progressive improvements. Regular assessment of strength deficit should be made to determine if training should be more hypertrophy or RFD oriented. It should have a special emphasis on possible muscular imbalances due to the higher levels of intensity and volume related to tennis training and tournaments | ||
| Adulthood | The training should be regular and lead to progressive improvements. However, training should spot imbalances, inadequacies and weak points of the athletes in order to optimize performance in tennis in the long term. | ||
Conclusion
In short, a strength training program should consist of integration of stability and recovery / corrective exercises, together with strength work of both maximal and explosive characteristics, as well as court work focusing strength components such as speed, agility and power.
References
Balyi, I. & Hamilton, A. (1999). The FUNdamentals in Long-term Preparation of Tennis Players. In N. Bollettieri (Ed.). Nick Bolletieri Classic Tennis Handbook, (pp. 258-280). New York: Tennis Week.
Folkins, C. H. & Sime, M. E. (1981). Physical training and mental helath. Journal of Physiology, 36, 373-389.
Fox, E.L. (1984). Sports Physiology (2nd edition). Philadelphia: W.B. Saunders.
Jensen, C. R. & Fisher, A. G. (1979). Scientific Basis of Athletic Conditioning. Philadelphia: Lea & Fegiber.
Kibler, W. B. & Chandler, T. J. (1994). Raquet Sports. In F.Fu &D. Stone (Eds.), Sports injuries: Mecahnisms, Prevention, and Treatment. Baltimore: Williams & Williams.
Lamb, D. R. (1984). Physiology of Exercise (2nd edition). New York: MacMilan.
O’Shea, J. P. (1976). Scientific principles and Methods of Strength Fitness (2nd edition). Reading: Addison.Wesley.
O’Sullivan, S. B. & Schmitz, T.J. (1998). Strategies to improve motor control and motor learning. Physical Reabilitation: Assessment and Treatement (3rd edition) (pp.225-244). Philadelphia: F.A. davis.
Rasch, P. J. (1979). Weight Training (3rd edition). Duduque: Wm. C. Brown.
Stone, M. H., Byrd, R., Carter, D. et al. (1982). Physiological effects of short-term resistive training on middle-age sedentary men. National Strength and Conditioning Association Journal, 4, 5, 16-20.
Tucker, L. A. (1983). Self Concept: Afunction of self-perceived somatotype. Journal of Psycology, 113, 123-133.
Verstegen, M. (2003). ITF Strength & Conditioning for Tennis. In M. Reid, A. Quinn, & M. Crespo (Eds), Developing strength (pp. 113-135). London: ITF Ltd.

O Trenó é um equipamento extremamente versátil que possibilita treinar uma grande variedade de exercícios. A sua utilização é relativamente simples, uma vez que não é tão técnico em relação a muitos outros exercícios, o que faz com que seja possível progredir e obter resultados de forma rápida e segura.
A sua versatilidade permite que seja utilizado com vista ao desenvolvimento de inúmeros objetivos como potência, força, hipertrofia, endurance ou perda de massa gorda, modificando variáveis como a carga, intervalos de tempo, distâncias percorridas e períodos de descanso (atendendo às necessidades fisiológicas do objetivo que se pretende atingir).
As infindáveis variantes que permite realizar faz com que seja uma opção viável quando se pretende incrementar intensidade no treino em praticantes que possam ter algumas limitações, não tolerando exercícios de alto impacto e/ou carga axial.
Para além de todas as razões anteriormente referidas, seguem-se alguns aspetos em que a utilização do trenó pode ser bastante benéfica.
RECUPERAÇÃO ATIVA: Quando realizado com intensidades relativamente baixas é uma ótima forma de aumentar o fluxo sanguíneo nos tecidos ativos com o intuito de promover o processo de regeneração. Os exercícios realizados com o trenó exigem essencialmente ações musculares de natureza concêntrica, resultando num menor número de microlesões em resposta à sobrecarga mecânica, sobretudo quando comparado com outros exercícios de força com predomínio de ações excêntricas. Dessa forma é possível aumentar o fluxo sanguíneo junto dos tecidos em regeneração sem induzir dano muscular, diminuindo assim o período de recuperação.
ACELERAÇÃO: A literatura atual tem apontado a aceleração como um fator determinante no rendimento desportivo. A aceleração é bastante dependente da fase inicial de um sprint, onde a capacidade de realizar um primeiro contacto com o solo de forma explosiva influenciará amplamente a aceleração subsequente. A utilização do trenó, quer pela similaridade de ângulos articulares presentes na técnica de corrida, quer pelo carácter contralateral, em que as forças de reação ao solo são transmitidas de forma unilateral, fazem com que este seja uma ótima opção quando se pretende criar passadas mais rápidas e fortes melhorando a capacidade de acelerar em todas as direções.
REABILITAÇÃO/PREVENÇÃO DE LESÕES: Algumas variantes como o Backward Sled Drag permitem incidir de forma eficaz sobre os quadríceps, realizando a extensão do joelho em pé, em indivíduos que se encontram a recuperar de uma lesão. Esta variante possibilita o trabalho nos últimos graus de extensão do joelho sem uma elevada carga excêntrica sobre os tecidos e sobrecarga da articulação.
Desta forma o trenó tem lugar em programas de treino de força e condição física, reabilitação e prevenção de lesões, sendo possível adequar a sua utilização em prol do objetivo pretendido para praticamente todos os níveis de aptidão física.
Bons treinos!
Patrick Filipe

O Press é uma excelente “ferramenta” para construir força e massa muscular ao nível da parte superior do corpo. Está presente em muitos programas de treino de força e condição física, sobretudo no contexto desportivo. Seguem-se algumas das razões pelo qual este deve fazer parte de um programa de treino de força, para além de construir ombros grandes e fortes!
1) DESENVOLVIMENTO MUSCULAR: O Press é um dos exercícios mais efetivos para um desenvolvimento equilibrado da cintura escapular. Apesar do seu foco ser predominantemente no deltóide anterior, este também envolve o deltóide medial e posterior. Além do deltóide também o trapézio é fortemente envolvido na execução, sobretudo no momento do bloqueio final do movimento (Lockout) em que é necessário estabilizar a barra, impedindo que esta se desloque para a frente ou para trás.
2) ESTABILIDADE DO TRONCO: A execução do Press é extremamente exigente para os músculos estabilizadores do tronco. Uma revisão sistemática da literatura (Martuscello et al., 2012) demonstrou, através da atividade eletromiográfica dos músculos estabilizadores do tronco, que exercícios como Agachamento, Peso Morto e Press são mais efetivos quando comparados com exercícios “específicos” para a estabilização do tronco como Abdominal Crunch ou Prancha (com/sem plataformas instáveis).
3) MELHORIAS NO SUPINO: Uma das melhores formas de alcançar uma execução sólida no supino é através da realização do Press. O Press exige uma maior ativação da musculatura da parte superior das costas, fortalecendo músculos responsáveis pela fase excêntrica do supino, sendo esta de extrema importância para a conclusão do movimento. Devido a vários mecanismos de inibição, a progressão ao nível do supino é muitas vezes bloqueada, podendo levar a longos períodos de estagnação. Ed Coan, uma lenda no Mundo do Powerlifting, afirmou ter quebrado um longo período de estagnação após a inclusão do Press na sua rotina de treino.
4) TRANSFER: O Press é um dos exercícios mais vantajosos ao nível dos membros superiores devido ao transfer positivo em inúmeras habilidades no contexto desportivo. A grande maioria das modalidades desportivas exigem o uso da força dos membros superiores para transmitir essa força ao longo de uma cadeia cinética que tem início no chão. Sempre que um atleta empurra um oponente, lança um objeto ou usa uma raquete ou taco para transmitir força para determinado objeto, a força tem início com os pés contra o chão. A força produzida durante a execução do Press não é exclusiva dos membros superiores, envolve todo o corpo de forma a proporcionar a estabilização necessária, ou seja, a produção e transmissão de força entre a base de suporte e a carga movida inicia-se no chão e termina na barra nas mãos.
No entanto, a sua execução é complexa e exigente, é necessário garantir que todas as estruturas envolvidas têm a capacidade para realizar o movimento ao longo de toda a amplitude. Desta forma é possível aprender, consolidar e incrementar carga com segurança, beneficiando de todas as vantagens anteriormente referidas. Para saber se está apto a introduzir o Press nos seus treinos procure o aconselhamento de um profissional qualificado.
Patrick Filipe
Referências:
Saeterbakken, A.H. Fimland, M.S. Effects of Body Position and Loading Modality on Muscle Activity and Strength in Shoulder Presses. Journal of Strength and Conditioning Research 2013, 27, 7, 1824-1831.
Martuscello, J. (2013). Systematic review of core muscle activity during physical fitness exercises. J Strength Cond Res 27(6)/1684-1698.
Rippetoe, M., & Kilgore, L. (2011). Starting Strength: Basic Barbell Training. 3rd ed. Wichita Falls, TX: Aasgaard Co.

O Farmer´s Walk pode ser uma “ferramenta” poderosa quando se pretende desenvolver qualidades físicas. Devido à sua versatilidade este pode ser utilizado por qualquer pessoa, seja com o objetivo de ficar mais forte, aumentar a massa muscular e/ou perda de massa gorda. A sua execução é simples: mantenha o tronco e cabeça em posição neutra com o olhar dirigido para a frente, enquanto mantém os ombros ligeiramente retraídos e deprimidos. Contraia os glúteos e abdominais enquanto dá passos curtos, mas rápidos. Passos mais amplos farão oscilar o peso tornando a caminhada instável.
Contudo os seus benefícios vão muito mais além dos anteriormente mencionados! De que forma?
FORÇA DE PREENSÃO: A força de preensão está correlacionada com a força dos membros superiores, força geral do corpo, capacidade funcional e tem um impacto direto sobre o desempenho no treino. Para Gray Cook (2010) este é um dos muitos exercícios classificados como “self-limiting exercise”, ou seja, são autolimitados pela respiração, força de preensão, equilíbrio, postura e coordenação. Alguns exercícios, como o Farmer’s Walk combinam várias características auto-limitantes, sendo a força de preensão a mais decisiva devido ao tempo em que é necessário suportar a carga nas mãos, aspeto que muitas vezes é o fator limitante durante a execução de exercícios com o Peso Morto.
PADRÃO DE MARCHA: Um estudo de Winwood et al. (2014) sugere que o Farmer´s Walk pode ser um estímulo mecânico eficiente na melhoria de vários aspetos do ciclo de marcha. As adaptações neuromusculares, como melhorias na produção de forças propulsoras anteriores e verticais, força e estabilidade do tornozelo, desenvolvimento da cadeia cinética dos membros inferiores e estabilização do tronco, fazem deste uma ótima opção para a melhoria da condição física geral.
ESTABILIDADE DO TRONCO: Segundo o Dr. Stuart McGill (2009) a solicitação muscular que é necessária para manter uma postura vertical, estabilizando o tronco durante a caminhada, incidirá sobre os músculos estabilizadores do tronco como nenhum outro exercício. Quando realizado unilateralmente este tem um caráter de anti-rotação e flexão, fazendo com que os estabilizadores do tronco atuem contra o peso, evitando que o tronco rode e flexione para o lado que transporta a carga. Músculos como o quadrado lombar e os oblíquos têm um papel preponderante para a produção de força no plano frontal, conferindo estabilidade ao tronco e pélvis, auxiliando a coxa durante a produção de força em tarefas como a corrida, mudanças de direção e levantamentos básicos.
É um “finisher” por excelência com uma ampla variedade de aplicações que impulsionam a capacidade de trabalho e condição física para outro nível. Não subestime o impacto deste exercício simples, mas não simplista!
Patrick Filipe
Referências:
Cook, G., Burton, L., Kiesel, K., Rose, G., Bryant, M. (2010). Functional Movement Systems: Screening, Assessment, Corrective Strategies. Santa Cruz, California. On Target Publications.
Winwood, P.W., Cronin, J.B., Cowan, E., Keogh, J. (2014). A biomechanical analysis of the farmers walk, and comparison with the deadlift and unloaded Walk. International Journal of Sports Science Coaching. 9 (5):. 1127-1143.
McGill, S.M., McDermott, A., Fenwick, C.M.J. (2009). Comparison of different strongman events: trunk muscle activation and lumbar spine motion, load, and stiffness. Journal of Strength and Conditioning Research 23(4):. 1148–1161.

Um dos mais sérios problemas de saúde pública na Europa é a obesidade. A sua prevalência atingiu proporções epidémicas, pois triplicou nas últimas duas décadas. Segundo a World Health Organization (WHO) em 2010, existiam 15 milhões de crianças e adolescentes que teriam obesidade. Diversas patologias estão associadas à obesidade como a diabetes mellitus tipo 2, doenças cardiovasculares e, mais recentemente, a síndrome metabólica que conjuga os seguintes fatores de risco: obesidade abdominal, hipertensão, dislipidémia e resistência à insulina. Esta doença afeta entre 20 a 30% da população total da Europa (WHO, 2007).
Segundo a revisão de Lobstein, Baur, & Uauy (2004), estima-se que 10% das crianças em idade escolar (5 – 17 anos) em todo o mundo apresentam excesso de peso. Na Europa os valores são ainda mais alarmantes, pois a prevalência atinge os 20%.
Em Portugal, considerando as crianças entre os 7 e 9 anos de idade a taxa de prevalência é a mais elevada de toda a Europa (32%). A epidemia da obesidade tem vindo a progredir de forma alarmante e concluiu-se que aproximadamente 38% das crianças europeias em idade escolar tenham excesso de peso e que mais de um quarto apresentavam obesidade (WHO, 2007).
O treino de força (TF) tem ganho popularidade entre os adolescentes com obesidade. Através de uma correcta prescrição e supervisão, estes programas de exercício são um método seguro de desenvolvimento da força muscular (Nowicka & Flodmark, 2007; Wafs, Jones, Davis, & Green, 2005). Seguindo uma progressão apropriada do volume e intensidade de treino, os adolescentes com obesidade poderão ter sucesso e divertir-se (Nowicka & Flodmark, 2007; Wafs et al., 2005).
O TF ajuda a desenvolver a massa isenta de gordura (MIG) e a atenuar o decréscimo da taxa metabólica de repouso que ocorre em algumas estratégias alimentares de perda de peso corporal (Wafs et al., 2005).
Embora o TF não seja caracterizado por um elevado dispêndio energético, este tipo de exercício é uma componente importante de um programa de perda de peso, pois além de melhorar a força e resistência musculares, influencia positivamente a densidade mineral óssea, a capacidade cardiorrespiratória, a dislipidémia e a composição corporal (Faigenbaum, 2007; Faigenbaum & Westcof, 2007).
Os adolescentes com obesidade apresentam alguma relutância em permanecerem activos devido às dificuldades motoras causadas pelo elevado peso corporal. Daí, considerarem as actividades aeróbias como aborrecidas e desconfortáveis (Faigenbaum & Westcof, 2007; Faigenbaum et al., 2007). No entanto, parecem apreciar o treino de força, porque este caracteriza-se por períodos curtos de esforço, seguidos de uma pequena pausa entre séries ou exercícios. Ao contrário do que acontece com o exercício aeróbio, a sua forma intervalada e não contínua é semelhante aos movimentos e deslocamentos realizados pelas crianças e adolescentes quando jogam e brincam (Faigenbaum & Westcof, 2007; Faigenbaum et al., 2007).
Os jovens com obesidade, por norma, são os mais fortes da turma e recebem feedback positivo, devido à sua capacidade de levantar cargas elevadas nos exercícios de força. Ao contrário do exercício aeróbio contínuo, a participação num TF dá a possibilidade destes jovens se destacarem positivamente perante os colegas com peso saudável. Assim, ganham confiança e motivação para se tornarem mais activos (Faigenbaum & Westcof, 2007; Faigenbaum et al., 2007).
Pedro Ribeiro
Referências:
Faigenbaum, A. D. (2007). State of the Art Reviews: Resistance Training for Children and Adolescents: Are There Health Outcomes? American Journal of Lifestyle Medicine, 1(3), 190–200. doi:10.1177/1559827606296814.
Faigenbaum, A. D., & Westcof, W. L. (2007). Resistance Training for Obese Children and Adolescents. President’s Council on Physical Fitness and Sports – Research Digest, (3), 2–8.
Lobstein, T., Baur, L., & Uauy, R. (2004). Obesity in children and young people: a crisis in public health. Obesity Reviews, 5(1), 4–85.
Marshall, W. a., & Tanner, J. M. (1969). Variations in pattern of pubertal changes in girls. Archives of Disease in Childhood, 44(235), 291–303. doi:10.1136/adc.44.235.291.
Nowicka, P., & Flodmark, C.-E. (2007). Physical activity-key issues in treatment of childhood obesity. Acta Paediatrica, 96(454), 39–45. doi:10.1111/j.1651-2227.2007.00169.x
Wafs, K., Jones, T. W., Davis, E. A., & Green, D. (2005). Exercise Training in Obese Children. Sports Medicine, 35(5), 375–392.
World Health Organization. (2007). The challenge in the WHO European Region and the strategies for response: summary. (F. Branca, H. Nikogosian, & T. Lobstein, Eds.). World Health Organization Europe.

Esta é uma questão que parece ainda levantar muitas dúvidas entre as pessoas mas a verdade é que qualquer pessoa, de qualquer idade, pode ficar mais forte e melhorar a sua qualidade de vida. O processo de prescrição de treino é que será o factor crítico. Vamos ver um exemplo de um trabalho realizado com indivíduos com mais de 80 anos.
De acordo com este estudo publicado num jornal de Gerontologia, o treino de força (em conjunto com suplementação proteica) aumentou a massa muscular e força em indivíduos com idades compreendidas entre os 83 e 94 anos. O protocolo de treino foi realizado durante 12 semanas com três treinos por semana.
Mas há uma nota importante a registar. Apesar do aumento na força máxima de extensão do joelho e do aumento da área de secção transversal dos quadricípites, os investigadores não verificaram um aumento da capacidade funcional dos indivíduos, medida através de vários testes. Isto aconteceu, provavelmente, porque o protocolo de treino foi baseado em máquinas.
O protocolo de treino consistia de leg press, leg extensions, leg curls, dois exercícios para a parte superior do corpo (não identificados) e progrediu de 3 séries de 12 repetições para 5 séries de 6 repetições em 10 semanas seguidas depois de duas semanas de taper.
Em conclusão, apesar de ser positivo o aumento da massa muscular em indivíduos com estas idades, seria mais importante que houvesse uma maior transição funcional para as suas actividades diárias e nós acreditamos que isto teria acontecido se no protocolo de treino estivessem presentes exercícios como o agachamento, peso morto e empurrar o trenó – não é por acaso que estes exercícios são considerados um “must” nos programas de treino da The Strength Clinic.
Portanto, TREINO DE FORÇA sim, mas sempre na DOSE CERTA e com a MELHOR PROGRAMAÇÃO.
Bons treinos!
Pedro Correia
Referências:
Bechshøft RL, Malmgaard-Clausen NM, Gliese B, Beyer N, Mackey AL, Andersen JL, Kjær M, Holm L. Improved skeletal muscle mass and strength after heavy strength training in very old individuals. Exp Gerontol. 2017 Jun;92:96-105. doi: 10.1016/j.exger.2017.03.014. Epub 2017 Mar 28. PubMed PMID: 28363433.

O treino de força tem vindo a ser reconhecido como a estratégia de eleição para nos mantermos mais funcionais e durante mais tempo. Os benefícios do treino de força são de facto ubíquos e afectam positivamente os vários sistemas biológicos que tendem a decair com o envelhecimento, nomeadamente sistemas relacionados com as funções neuromuscular, cardiovascular e cognitiva.
Tem vindo a ser observado que protocolos de treino de força em que os exercícios incluídos são executados a maiores intensidades (>80% da máxima intensidade) ou com cargas mais leves mas executados de forma explosiva tendem a produzir melhores resultados quando comparados com protocolos de treino a intensidades mais baixas e/ou de forma não-explosiva (Mendonça et al., 2016a). Esta dinâmica das cargas (i.e. pesadas ou mais leves mas movimentadas de forma explosiva) são especialmente relevantes para populações mais idosas. Porquê? Porque o envelhecimento está associado à perda de fibras musculares Tipo II, que são as responsáveis pela produção de níveis de força máxima e explosiva. Ora, a esmagadora maioria dos movimentos da vida diária são de natureza balística (i.e. movimentos rápidos, de curta duração) e frequentemente com o objectivo de movimentar objectos relativamente pesados durante pouco tempo. Logo, não é de estranhar que um programa de treino que inclua uma dinâmica da carga de características pesada e/ou explosiva seja mais eficaz em “preparar” as pessoas para as actividades do dia a dia. Treinar a intensidades mais elevadas num programa de treino baseado em padrões de movimento fundamentais (agachar, empurrar, puxar, carregar e levantar objectos do chão) torna as pessoas menos vulneráveis a quedas, “maus jeitos”, e, ao mesmo tempo, mais capazes de recuperar desses incidentes caso ocorram.
Treine pesado e com inteligência! Um programa de treino estruturado respeitando o princípio da carga progressiva é mais valioso do que um programa que o mantém sempre dentro da zona de conforto. Seja o mais activo que conseguir durante o dia mas SE FOR TREINAR AO GINÁSIO NÃO PERCA TEMPO, TREINE MESMO! A sério, resulta!
Bons treinos!
Nuno Correia
Referências:
Mendonca, G. V. et al., 2016a. Impact of Exercise Training On Physiological Measures of Physical Fitness in the Elderly. Current aging science, 9(3).

É muito frequente ouvir relatos de pessoas que passam horas e horas no ginásio e continuam iguais. Não perdem gordura, não ganham massa magra, não ganham força, nem melhoram a sua capacidade funcional. Simplesmente não evoluem. Também temos aqueles que apostam apenas na componente do treino de musculação tradicional para emagrecer e mesmo assim nem sempre têm resultados, independentemente da alimentação que praticam.
Então, qual é o segredo para ter resultados? A programação do treino e a supervisão profissional talvez seja mais importante do que pensa.
No estudo efectuado por Bea et al. (2010), os autores investigaram a associação da frequência do exercício e do volume (peso total levantado no military press e nos agachamentos) com as alterações na composição corporal em mulheres no período pós menopausa que participaram num programa de treino de força progressivo durante seis anos.
As mulheres foram divididas em três grupos: um grupo fez treino de força durante esse período, um começou a fazer treino de força passado um ano e o terceiro (grupo controle) não fez nada. Os programas de treino foram supervisionados por profissionais e envolveram estratégias motivacionais para aumentar a adesão. O programa de treino contemplava oito exercícios (baseados em pesos livres e máquinas) e foi feito três vezes por semana, de forma progressiva.
Os resultados mostraram que apenas o grupo que não fez nada (grupo controle) ganhou peso e gordura ao longo dos seis anos, sugerindo algo que todas as pessoas já deviam saber: se não for feito nada em contrário (ao nível do exercício físico e do estilo de vida em geral) a cada dia que passa vamos ficar mais gordos e fracos.
Mas há ainda algo mais interessante a destacar. Os autores analisaram a relação entre a gordura corporal e o aumento de carga no agachamento e verificaram que as mulheres que ganharam mais força foram as que controlaram melhor o seu peso e a sua composição corporal ao longo do tempo! Ou seja, isto significa que se você está sempre a fazer o mesmo programa, sem atender às variáveis e princípios do treino, o mais certo é a estagnação.
Portanto, aquilo que temos para lhe dizer é que se faz parte daquele pacote que passa horas no ginásio, entre umas máquinas, selfies e conversa com o parceiro do lado, então não estará certamente no caminho para ter bons resultados. Sabemos que a parte da socialização é importante e que não deve ser ignorada, simplesmente cremos que deve ser bem gerida! O fulcral está em saber distinguir muito bem o que é treinar e o que é “ir ao ginásio”. E mais tempo a treinar é um indicador quantitativo, não é um indicador de qualidade.
Bons treinos!
Pedro Correia
Referências:
Bea JW, Cussler EC, Going SB, Blew RM, Metcalfe LL, Lohman TG. Resistance Training Predicts Six-Year Body Composition Change in Postmenopausal Women. Medicine and science in sports and exercise. 2010;42(7):1286-1295. doi:10.1249/MSS.0b013e3181ca8115.

O carácter profilático do exercício físico intenso e em particular do treino de força é cada vez mais reconhecido. De facto, é difícil encontrar um “comprimido” ou “medicamento” com um impacto positivo tão significativo em todos os órgãos e sistemas do nosso corpo. Contudo, muitas dúvidas e informação errónea existe quanto à segurança do treino de força com pessoas em condições de maior fragilidade, como por exemplo pessoas que se encontram doentes ou que foram recentemente sujeitas a tratamentos debilitantes. Os doentes oncológicos enquadram-se neste perfil, pois a doença em si é debilitante e os tratamentos seguidos (quimioterapia e radioterapia) podem ser muito debilitantes e indutores de efeitos secundários adversos.
Um exemplo comum destes casos é a ocorrência de linfedema no contexto do cancro da mama. Num estudo recente (referência e link abaixo), Simonavice et al. (2017) conduziu um programa de treino de força de 6 meses envolvendo grandes grupos musculares em mulheres (64 ± 7 anos de idade) sobreviventes de cancro da mama. A circunferência do braço foi avaliada para medir o aumento hipotético do linfedema. Não só não houve agravamento do linfedema nem a ocorrência de quaisquer outros eventos adversos, como o programa de treino de força resultou em aumento da força muscular, função física e qualidade de vida. Isso está de acordo com outros relatórios que mostram que os sobreviventes de cancro de mama podem e devem integrar programas de treino de força com intensidades moderada a alta para melhorar a força muscular, massa magra e densidade mineral óssea.
Na verdade, a contracção muscular é apontada como um mecanismo subjacente que serve como uma “bomba muscular” que, teoricamente, pode melhorar a drenagem do líquido linfático e potencialmente diminuir o risco de desenvolvimento de linfedema ou melhorar essa condição. Importante notar que as intensidades moderadas a altas implementadas de forma progressiva parecem oferecer mais benefícios.
Na The Strength Clinic acreditamos que todos podem treinar. TODOS DEVEM TREINAR independentemente da sua condição clínica! Naturalmente que o ajustamento da carga e exercícios é chave, e é por isso que os nossos treinadores são altamente qualificados e estão empenhados em garantir a DOSE CERTA para o seu caso!
Bons treinos!
Nuno Correia
Referências:
Simonavice, E., Kim, J.-S. & Panton, L., 2017. Effects of resistance exercise in women with or at risk for breast cancer-related lymphedema. Supportive Care in Cancer, 25(1), pp.9–15.
Recentemente, a International Society of Sports Nutrition publicou um “position stand” (ver referência abaixo) acerca da segurança e eficácia da suplementação com creatina no contexto do exercício, desporto e medicina.
A suplementação com creatina, um dos mais populares e estudados suplementos nutricionais, tem de facto mostrado ser eficaz em melhorar a performance atlética (sobretudo em exercício de alta intensidade) e induzir adaptações ao treino relevantes. O aumento consequente das reservas intra-musculares de creatina (e fosfocreatina) facilita a resíntese rápida de ATP (“moeda de troca” energética essencial para quase todas as reacções no nosso corpo) e dessa forma contribui para melhorar a performance porque aumenta a capacidade de produção de força, trabalho muscular, acelera a recuperação e parece contribuir para prevenir lesões.
Contudo, a suplementação com creatina parece ser altamente segura e eficaz em atletas, não-atletas (entusiastas do exercício físico) e ainda em várias populações clínicas. De facto, vários estudos (ver artigo da ISSN, referência abaixo) apontam para benefícios na suplementação com creatina nas mais variadas populações e contextos clínicos, tais como:
– Acelerar a reabilitação de lesões (porque atenua a atrofia muscular);
– Protecção de lesões neuronais (medulares e cerebrais);
– Atenuar as consequências debilitantes em pessoas com síndromas congénitos de deficiência de síntese de creatina;
– Atenuar a progressão de doenças neurodegenerativas (e.g. doença de Huntington, doença de Parkinson, doenças mitocondriais, esclerose lateral amiotrófica);
– Prevenir e/ou melhorar a bioenergética em pacientes com isquemia do miocárdio ou vítimas de acidente vascular cerebral;
– Melhorar indicadores metabólicos e funcionais associados ao envelhecinento;
– Possível benefício durante a gravidez para o óptimo crescimento, desenvolvimento e saúde do feto.
Em conclusão, a creatina parece de facto ser um suplemento nutricional seguro e com benefícios para as mais variadas populações e idades.
Nuno Correia
Referências:
Kreider, R.B. et al., 2017. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14(1), p.18.

Uma das componentes que desempenha um papel muito importante na corrida e que é muitas vezes negligenciado é o treino de força. Algumas das razões pelas quais o treino de força é preterido em relação a outros prende-se com o receio no aumento do peso, com a falta de tempo, com a falta de conhecimento e, também, com o facto deste tipo de treino ainda não estar disseminado no seio da corrida de fundo. Muitos praticantes desta disciplina ainda pensam que o seu treino deve ser só correr.
Neste texto pretendemos alertar para a importância do treino de força na economia da corrida, algo que preocupa bastante os atletas, principalmente os que correm as distâncias mais longas. Numa revisão sistemática realizada por Denadai et al. (2017) no jornal Sports Medicine, procurou-se encontrar relação entre treino de força e a economia da corrida. Os investigadores concluíram que os atletas que se submeteram a treino de força durante 6 semanas conseguiram atingir 2% de economia de esforço enquanto que às 16 semanas de treino, essa economia chegou a valores de 8%. Ou seja, isto significa que valores mais altos de economia de esforço durante a corrida poderão ser atingidos se os atletas se submeterem, ainda durante mais tempo, a um programa de treino de força.
O protocolo de treino era constituído por treino de força com carga e treino explosivo, sendo que treino de força em isometria não produziu os mesmos efeitos.
Sendo assim, devemos concluir que para potenciarmos todas as nossas qualidades físicas que irão ser responsáveis pela melhoria das nossas prestações em corridas longas, devemos, obrigatoriamente, introduzir o treino de força no nosso planeamento.
Que a FORÇA esteja sempre convosco!
Tiago Marto
Referências:
Denadai BS, de Aguiar RA, de Lima LC, Greco CC, Caputo F. Explosive Training and Heavy Weight Training are Effective for Improving Running Economy in Endurance Athletes: A Systematic Review and Meta-Analysis. Sports Med. 2017 Mar;47(3):545-554. doi: 10.1007/s40279-016-0604-z. Review. PubMed PMID: 27497600.

A prevalência auto-relatada de dor no ombro está estimada entre 16-26% e esta é a terceira causa mais comum de desordem músculo-esquelética em consulta (ver referência abaixo). Factores físicos como os seus hábitos de exercício e a realização de movimentos repetitivos (de baixa e alta intensidade) em posições inadequadas pode resultar em lesão ou em dores crónicas.
Por este motivo, na The Strength Clinic, consideramos que existem quatro pilares fundamentais no funcionamento do ombro:
1) Respiração – Respirar adequadamente é muito importante para maximizar a performance. Uma pessoa normal respira em média mais de oito milhões de vezes por ano e o mais provável é que ela não o faça da forma mais eficiente. A maior parte das pessoas utiliza apenas uma pequena percentagem da capacidade do corpo para extrair oxigénio do ar para os pulmões porque tem tendência em respirar somente com a parte superior do corpo (respiração apical), em vez de realizarem uma respiração mais profunda a partir do músculo respiratório mais eficiente que nós temos, o diafragma.
2) Postura – Apesar de sobrevalorizada na maior parte das vezes, a postura de cada indivíduo pode ter influência no aparecimento de lesões e na prevalência de dor crónica. Principalmente quando falamos de actividades com alto impacto / cargas elevadas (nas quais a biomecânica assume uma importância fundamental) e dos hábitos diários de movimento que cada pessoa tem. Uma postura deficiente é normalmente o resultado de vários desequilíbrios estruturais, musculares e articulares, no entanto, é preciso referir que o nosso corpo tem uma capacidade de adaptação enorme e que a falta de movimento de qualidade é, provavelmente, o problema principal. Ao contrário do que possa pensar não há posturas perfeitas!
3) Grip – Há um fenómeno chamado irradiação, portanto quanto maior a força de preensão, maior a activação dos nervos e músculos ao longo da cadeia cinética. Como consequência haverá um aumento da eficiência neurológica e teremos os músculos da coifa dos rotadores (supraespinhoso, infraespinhoso, pequeno redondo, subescapular) a disparar da forma que devem e não da forma convencional. As mãos estão intimamente ligadas com o funcionamento do sistema fisiológico e neurológico mas, infelizmente, este é um fenómeno muito ignorado nos programas de treino de hoje em dia.
4) Posição das articulações – O treino de coifa dos rotadores apenas não vai assegurar a saúde funcional do seu ombro. A estabilidade das omoplatas, que depende da mobilidade da coluna torácica, é fundamental para assegurar que a cavidade glenóide está bem posicionada para as forças aplicadas. A estabilidade das ancas e do tronco é também necessária para servir de fundação para a posição e funcionamento das omoplatas. Ou seja, se o controle do eixo central for fraco é muito provável que as suas omoplatas sejam arrastadas para posições desfavoráveis e isso vai prejudicar a transmissão de força.
Portanto, qualquer estratégia que tenha como finalidade melhorar a funcionalidade do ombro deverá considerar estes quatro pilares porque um ombro aparentemente forte não é necessariamente um ombro estável e é a estabilidade que deve preceder a produção de força.
Pedro Correia
Referências:
Mitchell C, Adebajo A, Hay E, Carr A. Shoulder pain: diagnosis and management in primary care. BMJ: British Medical Journal. 2005;331(7525):1124-1128.