Given the times we live in, where social contact is limited, the promotion of online services in all professional areas proliferates. In fitness, it seems that it has suddenly been discovered that you can (and should) train every day and that you can train at home and/or on your own. It is incredible the explosion of posts on social media by personal trainers offering sequences of exercises for people to perform at home. We know that, for better health and resilience, it is essential to exercise every day, just as it is essential to eat well and maintain personal hygiene, but this has always been so and, therefore, it is not only a necessity of current times.
For this reason, posting an exercise line-up for everyone to perform is as valuable as posting a photo of a meal or of someone brushing their teeth. It serves as much to remind you that these activities are important, but the content is not, to a large extent, applicable to you reading this text. Much less when it comes to exercise. In fact, picking up the fork and knife to eat, or the act of brushing your teeth are less complex activities than performing most of the physical exercises that we often see proposed, let alone organizing them in a training session.
The health and resilience resulting from training is even more relevant in times of crisis such as the one we are experiencing now, but that health and resilience was mainly built months and years prior to this moment. Notably during those months and years that you consistently went to the gym to do your workout, often with personal sacrifice. It is hard to organize oneself in order to be able to train! We have family and work and it is sometimes difficult to reconcile all social and professional obligations with the time we choose to invest in our health and well-being, like in the case of training. Notice that now I’m using the term training.
Because many of you who are reading these lines have long understood the difference between “exercising” and training. Many of you have realized that “exercising” is better than nothing, but that training is at a higher level. Training is a process that requires the organization and management of a range of variables over time. It requires making a careful assessment of the initial condition, selecting specific exercises and the ways to perform them, observing and evaluating movement, and making the necessary adjustments (e.g. load, type and form of exercise execution) in order to ensure constant progression along the path towards health, performance and resilience. Training is not the same as ‘’doing exercises” always varied and without criteria just to maintain some physical activity. And because some of you understand this difference, you have come over the months and years that preceded today’s turbulent times to make organizational sacrifices in order to train. And you chose to invest a little more of your time and money, and regularly went to a gym to get a training service. A service in which a program is followed, the exercises are not chosen at random, and in which the progression in the loads used as well as the execution of the exercises is closely monitored by a coach.
All the benefits of personalized training are possible to obtain remotely via online. I believe that the in-person format will always be superior, but with good organization and commitment from both the coach and student, constant progression is possible, and this difference can be mitigated. How do we know this at The Strength Clinic? Because we’ve been doing it for years! In addition, personalized training followed online may even have some advantages over the face-to-face format, such as:
- Not having to go to the gym at any given time. This can be a great advantage for some people. If the self-discipline of following your training program is guaranteed, travel time and what it implies in organizational terms is saved. In addition, you can choose a training time slot that best fits your schedule without being conditioned by the availability of your coach;
- Greater consistency and commitment doing the exercises in your program. Since you can choose the time slot of your training session, you are less likely to miss it, as you will have more flexibility in adjusting the schedule if needed. This way, it is more likely that you reach the weekly training frequency that is desirable. In addition, as we recommend that you document on video a summary of each workout on an online platform so that your coach can observe, this also adds an additional sense of commitment to the session and the proper execution of the exercises;
- Better cost benefit. In fact, you will be able to enjoy almost all the benefits of having a personal trainer for a lower price because you will not have to pay for the running costs of the facility and its equipment usage where the in-person training session would take place;
- Train directly with your favorite coach. If the coach you would like to work with is not available in-person or his/her in-person rate is beyond your means, the online option will allow you to work directly with him for a lower price.
The message “don’t stop training even if you are at home or on your own” in the context of the crisis we are experiencing today is correct! However, this need did not arise today. It is something that should be part of our lives if we want to remain getting stronger and healthier forever. For this purpose, training is much better than just “exercising”, especially if you follow workouts taken from social media that do not take into account your specific profile, your body awareness and do not follow any criteria for exercise selection and future programming. It only serves the purpose of “moving the body” and getting tired in that moment or day, but it will not accomplish much more than that. Because training implies a process that is based on your goals and individual characteristics. In a training session, what you do today was based on what you did yesterday and what you are going to do in the future. And it is possible to continue to train online and reap all the benefits of personalized training, even at a distance. It requires a mutual commitment of the student and coach in a process that is joint. Your optimized personal development will always be our commitment at The Strength Clinic. We are here to guide you through this process rather that offering “one size fits all” workouts for everyone!
Stay strong!
Nuno Correia

The International Society of Sports Nutrition published in 2017 a position stand (see reference below) on the safety and efficacy of creatine supplementation in the context of exercise, sports and medicine.
Creatine supplementation, one of the most popular and studied nutritional supplements, has in fact been shown to be effective in improving athletic performance (especially in high intensity exercise) and inducing relevant training adaptations. The consequent increase in intramuscular creatine (and phosphocreatine) reserves facilitates the rapid re-synthesis of ATP, the so-called energy “currency” of the body, which is essential for almost every reaction in our body. Thus, the increased availability of creatine in the cell through supplementation contributes to improve performance because it increases the energy availability in order to exercise (i.e. muscle contraction) as well as a whole range of other muscle cell related reactions. Creatine supplementation can in fact enhance strength production, muscle work, accelerate recovery and help preventing injury.
Additionally, creatine supplementation appears to be highly safe and effective not only in athletes but also in non-athletes (such as the so-called exercise enthusiasts), as well as in various clinical populations. In fact, several studies (see ISSN article, reference below) point to benefits of creatine supplementation in various populations and clinical settings, such as:
– Accelerating injury rehabilitation (because it attenuates muscle atrophy);
– Protection of neuronal injuries (spinal and cerebral);
– Mitigation of debilitating consequences in people with congenital syndromes of creatine synthesis deficiency;
– Attenuating the progression of neurodegenerative diseases (e.g. Huntington’s disease, disease, Parkinson’s disease, mitochondrial diseases, amyotrophic lateral sclerosis);
– Prevention and / or improvement of bioenergetics in patients with myocardial ischemia or stroke victims;
– Improving metabolic and functional indicators associated with aging;
– Possible benefit during pregnancy for optimal growth, development and health of the fetus.
In conclusion, creatine does indeed appear to be a safe and beneficial nutritional supplement for a wide range of populations and ages. Indeed, this is a supplement that actually works!
Take creatine and power to you!
Nuno Correia
References:
Kreider, R.B. et al., 2017. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14(1), p.18. Available at: http://jissn.biomedcentral.com/articles/10.1186/s12970-017-0173-z.

“People don’t decide their future, people decide their habits and their habits decide their future.”
– F.M. Alexander
Nine years ago (2010)1, the European Working Group on Sarcopenia in Older People (EWGSOP) published a definition of sarcopenia that has been widely used worldwide and this definition has fostered advances in the identification and care of people at risk or with sarcopenia. It was defined as a syndrome characterized by progressive and widespread loss of muscle mass and strength at risk of adverse outcomes such as physical disability, poor quality of life and death. Because the relationship between muscle mass and strength is not linear (the ability to generate strength is not only dependent of muscle mass), the criteria for its diagnosis included low muscle mass and low muscle function (i.e. strength or physical performance).
After learning that in 2016 sarcopenia was classified as a disease by the World Health Organization, as noted in the first part of this article, the EWGSOP22 updated its operational definition and various diagnostic strategies, considering now that muscle strength (measured by grip strength or the chair stand test) is the main parameter for measuring muscle function, even more important than the amount of muscle mass. Therefore, it is in this context that we justify the title of this article and reinforce the importance of sharing this message with all health professionals.
The implications of this condition on human health are several and widely known: increased risk of falls and fractures3,4; impairment of activities of daily living5; association with heart disease6; respiratory disease7 and cognitive dysfunction8; lower quality of life9; loss of independence10,11,12 and death13. In financial terms, public health costs have also been calculated in several papers. In a study by Janssen et. al.14, in 2004, the costs of sarcopenia in the United States were estimated at $ 18.5 billion annually, representing about 1.5% of total health costs. In a study conducted here in Portugal at the Hospital de Santo António in Porto and published in 201615, it was found that hospitalization costs associated with sarcopenia were higher by 58.5% for patients under 65 years and by 34% for patients aged 65 and over. More recently (2018), the Hertfordshire Cohort Study in the United Kingdom16 found that the costs associated with lack of muscle strength were estimated at £ 2.5 billion annually.
In the present scenario, where the phenotype of unhealthy aging is proliferating in the eyes of all industrialized nations, in which diseases such as hypertension, cancer, depression, Alzheimer’s disease and type II diabetes are destroying people’s lives, it is essential to adopt measures aimed at improving function of each individual rather than diagnosing illnesses and administering medicines which, in addition, do not help solving this problem, and may further aggravate their condition. We know that the main health problems are related to poor diet, physical inactivity, lack of sleep, excess alcohol, exposure to tobacco and polluted environments but also lack of movement quality, vigor and muscular strength.
The benefits of strength training in health are well supported in the scientific literature and the most important ones are: decrease in blood pressure; decreased risk of osteoporosis and sarcopenia; improvement of lipid profile; increased cardiorespiratory capacity; prevention and management of chronic pain; increased insulin sensitivity; improvement of wellbeing and self-confidence. Moreover, several studies17,18,19 have shown a strong and consistent correlation between increased strength and muscle mass with decreased mortality, reinforcing the fact that the decline in strength associated with the current levels of sedentarism and aging need to be addressed. Therefore, a well-designed strength training program that meets the individual’s competency and follows the principles of adaptation to training will improve all of the above health indicators and all the necessary physical qualities (strength, power, speed, agility, balance, coordination, mobility, endurance) to carry out the activities of our daily life. These are the parameters of physical function that are currently being proposed as biomarkers of aging in humans20.
Consequently, program design will be the determining factor in this equation. And while it is true that this process requires imperative knowledge of sports sciences, it must be borne in mind that it also requires field work and art in coaching. Instead of being so preoccupied with following the guidelines and looking for statistically significant results, we should be concerned that our approach is relevant to one’s life. Because we work with people. People who have time constraints to train. People with different family and professional responsibilities. People who have different lives from each other. People who have a host of metabolic and / or orthopedic problems that no randomized controlled trial can ever reproduce! Yes, this is a complex process.
Finally, we know that one of the mechanisms responsible for muscle atrophy, sarcopenia and aging is apoptosis, a form of programmed cell death and a fundamental process in aging. But when we train, eat and rest properly, we are sending a signal to our body to create an anabolic environment, an environment that enhances the release of growth factors and suppresses apoptosis. That is, strength training is a macroscopic growth factor that suppresses programmed cell death (i.e. apoptosis), but unlike drugs, where an increasing in dose means more disease and dependence, an increase in load (even if reduced) means more health, more strength and more vigor. This way, the daily decisions will always be up to each one: treat the body like a Ferrari or treat the body like a rental car.
Pedro Correia
References:
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing 2010; 39: 412–23.
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jan 1;48(1):16-31.
- Bischoff-Ferrari HA, Orav JE, Kanis JA et al. Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos Int 2015; 26:2793–802.
- Schaap LA, van Schoor NM, Lips P et al. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: the longitudinal aging study Amsterdam. J Gerontol A Biol Sci Med Sci 2018; 73: 1199–204.
- Malmstrom TK, Miller DK, Simonsick EM et al. SARC-F: a symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J Cachexia Sarcopenia Muscle 2016; 7: 28–36.
- Bahat G, Ilhan B. Sarcopenia and the cardiometabolic syndrome: a narrative review. Eur Geriatr Med 2016; 6: 220–23.
- Bone AE, Hepgul N, Kon S et al. Sarcopenia and frailty in chronic respiratory disease. Chron Respir Dis 2017; 14: 85–99.
- Chang KV, Hsu TH, Wu WT et al. Association between sarcopenia and cognitive impairment: a systematic review and metaanalysis. J Am Med Dir Assoc 2016; 17: 1164.e7–64.e15.
- Beaudart C, Biver E, Reginster JY et al. Validation of the SarQoL(R), a specific health-related quality of life questionnaire for Sarcopenia. J Cachexia Sarcopenia Muscle 2017; 8: 238–44.
- Dos Santos L, Cyrino ES, Antunes M et al. Sarcopenia and physical independence in older adults: the independent and synergic role of muscle mass and muscle function. J Cachexia Sarcopenia Muscle 2017; 8: 245–50.
- Akune T, Muraki S, Oka H et al. Incidence of certified need of care in the long-term care insurance system and its risk factors in the elderly of Japanese population-based cohorts: the ROAD study. Geriatr Gerontol Int 2014; 14: 695–701.
- Steffl M, Bohannon RW, Sontakova L et al. Relationship between sarcopenia and physical activity in older people: a systematic review and meta-analysis. Clin Interv Aging 2017; 12: 835–45.
- De Buyser SL, Petrovic M, Taes YE et al. Validation of the FNIH sarcopenia criteria and SOF frailty index as predictors of long-term mortality in ambulatory older men. Age Ageing 2016; 45: 602–8.
- Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R. The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc. 2004 Jan;52(1):80-5.
- Sousa AS, Guerra RS, Fonseca I, Pichel F, Ferreira S, Amaral TF. Financial impact of sarcopenia on hospitalization costs. Eur J Clin Nutr. 2016 Sep;70(9):1046-51. doi: 10.1038/ejcn.2016.73. Epub 2016 May 11.
- Pinedo Villanueva, R. A., Westbury, L. D., Syddall, H. E., Sanchez, M., Dennison, E. M., Robinson, S. M., & Cooper, C. (2018). Health care costs associated with muscle weakness: a UK population-based estimate. Calcified Tissue International.
- Ruiz JR, Sui X, Lobelo F, et al. Association between muscular strength and mortality in men: prospective cohort study. BMJ. 2008;337(7661):a439. Published. doi:10.1136/bmj.a439.
- Srikanthan P, Karlamangla AS. Muscle mass index as a predictor of longevity in older adults. Am J Med. 2014;127(6):547-53.
- Dos Santos L, Cyrino ES, Antunes M, Santos DA, Sardinha LB. Changes in phase angle and body composition induced by resistance training in older women. Eur J Clin Nutr. 2016 Dec;70(12):1408-1413. doi: 10.1038/ejcn.2016.124. Epub 2016 Jul 13. PubMed PMID: 27406159.
- Cadore EL, Izquierdo M. Muscle Power Training: A Hallmark for Muscle Function Retaining in Frail Clinical Setting. J Am Med Dir Assoc. 2018 Mar;19(3):190-192.

There is currently sufficient scientific evidence to assert that strength training is an effective method for preventing, treating and potentially reversing various chronic diseases. Indeed, adherence to a properly designed strength training program can significantly increase the physical and mental health of the population.
The importance is such that several world-renowned organizations (World Health Organization, Centers for Disease Control and Prevention, American Heart Association, American Association for Cardiovascular and Pulmonary Rehabilitation, American College of Sports Medicine) recommend this form of training for maintain health.
However, despite this evidence, most of exercise recommendations are still for aerobic training, and few physicians (and health professionals in general) recommend strength training. This article aims to alert for the relevance and valuable impact of strength training on health.
About 100% of our biological existence has been dominated by outdoor activity. Hunting and searching for food has been a condition of human life for millions of years1. That is, if in the past it took effort (i.e. physical activity) to find food, nowadays food comes to us without having to make any effort. Therefore, we have moved from a very active lifestyle to a highly sedentary lifestyle. With serious consequences for public health. If in the past all people had to engage in some sort of physical exertion to carry out their daily tasks, today most of them do not have those needs. The environment has changed and so have people. They are weaker, sicker, have more chronic pain and are increasingly dependent on medicines. But the message still going on in our society (and passed on in medical appointments) is “make no physical efforts and follow your normal life”. And I believe this is the worst advice people can get! Normal life? But what kind of advice is this? How can normal be good? You must be completely alienated from reality in order to make such recommendations.
Today we have more opportunities than ever to build a healthy and strong phenotype. The phenotype is the expression of our organism, and it depends largely on the choices we make every day. Two organisms can have the same genotype, the same DNA, but different phenotypes – based on their experiences and the environment. Admittedly, there are things we cannot control such as our genetic heritage, the place of the world where we were born / lived, overall luck and the general environment to some extent. But there are many things that we can control that depend solely on our priorities in life and our daily choices (examples: exercise habits, eating, sleeping, stress management, smoking, alcohol, exposure to polluted environments). And I believe that exercise in general (and strength training in particular) is the most important factor of all. It is the most potent, it’s quantifiable and acts quickly on all systems and organs of the human body.
The reality is this: the population is aging and with more chronic / noncommunicable diseases. The main noncommunicable diseases are cardiovascular diseases, cancers, chronic respiratory diseases and diabetes. These four disease groups alone account for over 80% of the 41 million deaths in the world2! According to the first report on healthy aging by the World Health Organization (WHO), the number of people over 60 is expected to double by 20503, and it is in this context that we need to urgently intervene to promote motor autonomy and improve people’s functional capacity. Traditional recommendations for walking, swimming, Pilates, and “doing low effort activities” or “no physical effort” probably need to be reconsidered and properly contextualized.
It is in this context that strength training and athletic training play a key role. All people (athletes and non-athletes) need to train their physical qualities to live with quality and independently. After age 30, adults lose 3-8% of their muscle mass per decade. Over time, the loss of lean mass contributes to a decrease in muscle strength and power, which are important predictors of balance, falls and mortality4. In the case of the elderly, it is important to note that falls are the main cause of accidental death after age 65 and hip fractures are those that most affect their independence5.
When I speak of strength I mean the basis for interacting with the environment around us, the foundation for the development of other physical qualities (mobility, power, speed, agility, muscle endurance), the ability to produce strength against external resistance (it can be the floor or any other object) through muscle contractions. This is probably the most trainable capacity we have and the one that could have the greatest impact on improving our function, independence and functional longevity. Tasks such as brisk walking, sitting and rising from a chair, climbing stairs, maintaining balance, carrying luggage, or playing with children / grandchildren are examples of activities in our daily lives that require a minimal component of various manifestations of strength (maximum strength, power and strength endurance). Therefore, both strength and muscle (quality rather than quantity) are physical function related parameters that need to be taken care of in the quest for achieving a healthy aging phenotype.
These issues are even more important when we note that as of 1st of October 2016, in the tenth revision of the International Classification of Diseases (ICD-10), sarcopenia has been classified as a disease by WHO and has its own code (M62.84). This should lead to increased availability of diagnostic tools and increased enthusiasm for the pharmaceutical industry to develop drugs to combat sarcopenia6. But in my opinion, this also represents a great opportunity for exercise professionals to be able to help fighting this disease, as strength training (properly oriented of course) will be the most potent stimulus in its prevention and treatment.
Pedro Correia
References:
- Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Comprehensive Physiology. 2012;2(2):1143-1211. doi:10.1002/cphy.c110025.
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet, 2016; 388(10053):1659-1724.
- Beard JR, Officer A, de Carvalho IA, et al. The world report on ageing and health: A policy framework for healthy ageing. Lancet 2016;387:2145e2154.
- English KL, Paddon-Jones D. Protecting muscle mass and function in older adults during bed rest. Current Opinion in Clinical Nutrition and Metabolic Care. 2010;13(1):34-39. doi:10.1097/MCO.0b013e328333aa66.
- National Center for Injury Prevention and Control of the Centers for Disease Control and Prevention. Preventing Falls: A Guide to Implementing Effective Community-Based Fall Prevention Programs 2nd edition. Atlanta: 2015.
- Anker SD, Morley JE, von Haehling S. Welcome to the ICD-10 code for sarcopenia. J Cachexia Sarcopenia Muscle. 2016 Dec;7(5):512-514. Epub 2016 Oct 17. PubMed PMID: 27891296; PubMed Central PMCID: PMC5114626.

We often hear reports from people who spend hours and hours in the gym and remain the same. They do not lose fat, do not gain lean mass, do not gain strength, nor improve their functional capacity. They simply do not evolve. We also have those who rely only on the traditional weight training component to lose weight and yet not always have results, regardless of the diet they follow.
So, what is the secret for having results? Program design and professional supervision may be more important than you think.
In a study conducted by Bea et al. (2010), the authors investigated the association of exercise frequency and volume (total weight lifted on the military press and squat exercises) with changes in body composition in postmenopausal women who participated in a progressive strength training program for six years.
The women were divided into three groups: one group did strength training during this period, one started strength training after one year and the third (control group) did nothing. The training programs were supervised by professionals and involved motivational strategies to increase adherence. The training program consisted of eight exercises (based on free weights and machines) and was done three times a week, progressively.
The results showed that the group that did nothing (control group) gained weight and fat over the six years, suggesting something that everyone should already know: if nothing is done, we will get fatter and weaker with each passing day.
But there is something more interesting to highlight. The authors analyzed the relationship between body fat and increased squat load and found that the women who gained the most strength had better control of their weight and body composition over time! This means that if you are always doing the same program without managing training variables and principles, stagnation is what will happen.
So, what we have to tell you is that if you are part of that package that spends hours in the gym, between exercise machines, selfies and talking to your partner, then you are certainly not on your way to good results. We know that the socialization part is important and should not be ignored, we simply believe that it must be well managed! The key is knowing how to clearly distinguish what is training and what is ‘’going to the gym’’. And more training time is merely a quantitative indicator, not a quality indicator.
Enjoy your training!
Pedro Correia
References:
Bea JW, Cussler EC, Going SB, Blew RM, Metcalfe LL, Lohman TG. Resistance Training Predicts Six-Year Body Composition Change in Postmenopausal Women. Medicine and science in sports and exercise. 2010;42(7):1286-1295. doi:10.1249/MSS.0b013e3181ca8115.

Following up on the topic addressed in the last article, let’s talk today about a common swing characteristic that affects a lot of golfers and that can compromise their swing efficiency and their performance on the golf course: Early Extension.
What is Early Extension?
Early extension can be understood as an integral part of loss of posture, this happens when the player’s hip and spine begin to extend too early in the downswing, i.e. the hips and pelvis move towards the ball in the downswing. In practical terms, if your body is not prepared to perform an efficient golf swing while maintaining good posture throughout the movement, you will end up lifting the upper body (spine) and miss the necessary hip rotation at impact. Your hips play a key role in injury prevention and performance improvement. If you have poor hip mobility, sooner or later your lower back will complain (and you can be sure that this situation will not be very pleasant).
According to studies conducted by the Titleist Performance Institute, 64.3% of amateur golfers early extend
Players who early extend usually refer that they feel trapped during the downswing as if they had to shrug their arms to hit the ball. And it’s normal for that to be so because when you extend your hips too early on the downswing, the space that was supposed to be occupied by your arms and hands was occupied by the lower body. Therefore, the end result will be a blockage of the movement, since your arms and hands can’t get out of the way and will still be needed to hit the ball.
How can I diagnose?
An easy and simple way to check if you do early extension is with your Smart Phone (you probably already have applications that allow you to draw lines and analyze your swing). All you need to do is to ask a friend to film you in the direction of the swing line and capture its full motion from the starting position (setup). After having your swing recorded, compare the position of your pelvis in the initial position with the position of the pelvis in the position of impact, if you notice that it moved towards the direction of the ball is because you extended your hip too early. If this is not possible, you can always ask your golf teacher to help you, I am sure he will be happy to do that.
What are the physical limitations?
“If you’re not assessing, you’re just guessing” – Greg Rose
The physical limitations can be many and to determine the causes that are affecting you, it would be important to make a functional assessment with a professional who understands how your body should move and its relation to the golf swing. According to what I have observed in my practice, I would like to highlight the following:
- Limitations on performing a full squat with the arms extended overhead;
- Limitations in hip mobility (especially in internal rotation of the leading hip and in anterior or posterior pelvic tilt);
- Limitations in the ability to separate / disassociate the thorax from hips (X factor);
- Limitations in the ability to stabilize the pelvis because the glutes and core muscles are inhibited.
What can I do to improve?
Although the causes may vary from person to person, I’m pretty sure that if you do the following exercises, you will improve and increase your body’s functionality to play golf for a longer time. You only need 10 minutes a day.
- Myofascial Release with Roller Stick

Using a roller stick, look for the trigger points of your calf and massage the inner, central and outer sides of the muscle for 30 seconds in each area. The points that hurt you most are those that need more care. Yes, this exercise might be a little uncomfortable but it’s worth it.
- Glute Bridge with Leg Extension

Lying in the supine position, push your heels against the floor, tighten your glutes, and raise your hips to form a glute bridge, with your arms up. Once in this position, extend one leg and form a straight line between the shoulder, hip and heel. Hold this position for 20-30 seconds, always keeping your hips high. Change legs and repeat 5 times on each side.
- Squat with Overhead Arm Reach

In the squat position (with your heels on the floor and your knees out), raise one arm up, lift the other arm (always looking at your hand) and then raise both arms at the same time and return to the standing position. If you can not squat without raising your heels, you can use a rolled up towel or a board to keep your heels high. Do 2-3 sets and repeat 8-10 times.
- Assisted Squat wiht Medicine Ball

In the standing position, with your feet shoulder-width apart and slightly rotated out, hold a medicine ball (or a bucket full of balls) in front of your body, and begin to slowly lower your body into the squat position by keeping your back straight and without lifting your heels off the floor. Do 2-3 sets and repeat 10-12 times.
I believe that these exercises can be helpful to you, but remember: The swing you can do is directly related to what your body is prepared to do.
See you soon!
Pedro Correia

If you still exercise to “burn calories,” you have not yet realized the purpose of a physical training program and the importance that movement has in our lives. The least important thing about exercise is the number of calories you burn! And that’s what I’ll try to explain in this article.
The power of exercise goes far beyond calorie burning, caloric expenditure is just a (nice) side effect of the type of exercise we do. Exercise consists of potentiating the release of powerful molecules and hormones that “talk” to our body’s organs (it’s not just food that has this kind of influence), and that determines what’s going to happen. And usually, the higher the intensity, the more beneficial the hormonal response.
Therefore, a well-designed physical training program has more to do with increasing energy levels, movement precision, vigor, muscular strength, mobility, agility, speed, work capacity and with an improved hormonal profile.
The Calorie Fever
I still see a lot of people worried about the calories in their food, the calories they burn when they exercise, the calories they consume each day, and I ask: How did we get here? What kind of message is being propagated that made people so obsessed with calories? Is calorie counting that important? Let’s see.
In order to discover the amount of energy in food, scientists burn food samples in a bomb calorimeter. And, to my knowledge, a bomb calorimeter does not share the same physiology and genetic makeup as a human being. As far as I know, a bomb calorimeter does not depend on the functioning of the various systems in the human body which are the real players in the way energy is absorbed and used (examples: digestive, endocrine and nervous system). This way of thinking is most likely unsustainable and ineffective long-term. This way of thinking is too reductive and does not solve the main problem – people’s lack of education regarding the importance of what we eat throughout our lives. Is it just me who finds it strange that most people are more concerned about their cell phones, cars and computers than with the origin and composition of the food they eat?
In fact, just look around and you’ll acknowledge that this is not the path to follow!
It is true that if we have the goal of losing fat mass, we must create an energy deficit, that is, the balance between the amount of calories (energy) entering our body and the amount of energy (calories) burned, must be negative. That’s the number one rule in rigid weight loss programs and that’s why we see Biggest Loser contestants training several times a day.
(Note: I should remind you that the Biggest Loser is a contest in which the goal is to lose weight in the shortest time possible, it’s not a contest to see who gets out of there healthier – if this was the goal probably there was no audience).
However, there is a lot more to be said. There are good calories and bad calories. The foods we eat, besides having a certain number of calories (which can be very difficult to determine with accuracy and can be highly variable), also have different properties with respect to their composition of macronutrients (protein, fat, carbohydrates) and micronutrients (minerals, vitamins, phytochemicals). These bioactive properties and compounds are what makes the difference and what should be studied preferentially. In my way of looking at things, it is more logical to first check the functionality of food (i.e. how its nutrients work) and then look at its caloric density, which can also be more or less functional depending on the objectives, morphology and specific conditions of each individual.
(Note: If you still think low fat diets are the most suitable for weight loss check the following study published in 2003 in the New England Journal of Medicine here, where it was shown that people on a high-fat diet lost more weight as those on a low-fat diet, the diet generally recommended by leading health organizations. But, of course, adherence to the diet will be the most important factor).
Back to calories…
Because the absorption of these nutrients will depend on the functioning of our digestive system – which in turn is governed by the endocrine system (think of hormones) and the nervous system (think of neurotransmitters) – and the health of the organs involved in the digestion process (mouth, esophagus, stomach, pancreas, small intestine, large intestine, liver, gallbladder), it becomes easy to understand that the web of relationships in the human body is much more complex than simple calorie counting. Albert Einstein has a quote that fits perfectly here: “make everything as simple as possible, but not simpler.”
The Power of Exercise
Anyone that is minimally informed about exercise already knows that long distance aerobic training is not the best choice for improving body composition and may even have opposite effects (catabolic effects) due to the pronounced increase in cortisol levels.
This has been known for a long time but it’s always important to remember. This study published by Tremblay, Simoneau and Bouchard in 1994, showed that the group that did 15 weeks of interval training burned NINE TIMES more fat than the group that did aerobic training. And this was in half of the time period!
What you need to “burn calories” is to increase the intensity of your workouts for certain periods of time, it’s this type of stimulus that will increase your metabolism and accelerate fat loss. In this study, a 30-minute training session of metabolic resistance training caused a 38-hour increase in metabolism – the famous afterburn effect or EPOC (post-exercise oxygen consumption). Let’s put this into perspective. Let’s say you trained this way on Friday morning. With this training method your body will still be in a “fat burning” mode on Saturday night, when you’re having dinner with your friends or with your boyfriend / girlfriend.
And why do I insist on combining a good diet with good training? Because I’m aware of the evidence on this topic. This study from 1999 showed that those who did aerobic training and strength training on a low calorie diet burned 44% more fat than those who merely followed dietary guidelines. As I’ve been saying, diet is the most important component for those people who want to lose fat, however, once that aspect is assured, only strength training and interval training can actually bring your results to a higher level. In my opinion, the fact that this study was based on a low-calorie diet combined with aerobic training is limiting, but we have to bear in mind that these are usually the guidelines of the American College of Sports Medicine (ACSM). The guidelines are intended to facilitate nutritional guidance offered by practitioners, but unfortunately that is not what I have observed when I discuss these issues with some colleagues.
I think you have already realized that the type of training you do can be a great ally to put your body in an energy deficit and consequently in fat burning status. Now I will try to explain why this is the least important of all. Stay with me!
Like nutrition, physical exercise is key to improve health, performance and body composition. You’re probably tired of hearing this. But it’s not any kind of physical exercise that works. Doing hundreds of crunches to lose belly fat, using all the gym machinery, running 10 miles a day, doing Pilates twice a week and doing 100 power cleans in the shortest time possible is not enough. You can call it physical exercise if you want, but it’s not just this kind of physical exercise our body needs. A more comprehensive approach is needed.
We need Good Movement (we shouldn’t start running in the first place)
The concept of “move more for your health” is insufficient for our real needs and to improve quality of life. We need good movement, we need to acquire movement competency in the first place. I am talking about the ability to perform fundamental movements with good form. Fundamental movement patterns such as squatting, hinging, pushing, pulling, throwing, carrying, walking, running and jumping.
From my point of view, running should be the last step in this process and yet what we most frequently see is people running all crooked and with an obvious deficit in muscle strength. But the problem is not theirs, they are trying to do something for their health (and probably that’s all they know), the problem is that most of them are not aware that running is a skill, which requires preparation, practice and training. Cristiano Ronaldo did not become the best player in the World over night, it took many hours of training (in the field and in the gym) to reach this level. Although it’s relatively easy and affordable for anyone to put on their shoes and just go out for a run, running also requires preparation, practice and training (technical and physical).
It is necessary to have stability, mobility, strength (every step we take on the ground is subject to the action of gravity and the speed we run, generating reaction forces of 2 to 5 times our body weight), symmetry, quality of movement and good musculoskeletal health. Running to get healthy or fit is one of the greatest physical distresses on our body if we don’t have a solid foundation. First, you need to be in good shape to run. If you don’t hone good movement skills, you are more likely to get injured. According to the available literature, the incidence rate of injury in runners may exceed 90%, this is more than any other sport. Plantar fasciitis, stress fractures, patellar tendonitis and patellofemoral pain are just a few examples. Check this systematic review if you’re interested in learning more.
Again, don’t get me wrong, I’m not anti-running and I admire the effort and suffering capacity of all runners. I think we should all be able to run (by the way, that’s how we evolved as a species), the problem is that most people who run are not properly prepared to run and there are fundamental learning steps that should not be overlooked in order to prevent structural imbalances in the musculoskeletal system and injuries. Cleary the simplistic idea of “move more” is not enough.
A new way to look at training
Different types of training can affect the way our genes work and how they interact with our cells. With good training it’s possible to decrease chronic inflammation, improve insulin sensitivity, strengthen the cardiovascular system, improve lipid profile, slow down normal aging, burn fat (as we’ve seen in more detail above), increase confidence and self-esteem, increase energy levels, increase mental strength, improve a number of physical skills that we need for our daily life activities or sports practice (such as strength, stability, mobility, balance, speed, agility) and our different energy systems (ATP-CP, glycolytic, and oxidative). As we age, these skills naturally decline, but the fact is that with a more comprehensive training program it is possible to reverse and / or at least mitigate this decline.
Most people think that genes are the brain of the cell, they believe that if genes don’t tell you what to do, the cell dies. But if you remove the genes from the cell, the cell is still alive, eliminating waste products and behaving just like another cell. So, instead of genes being the brain of the cell, think of genes as your instruction / repair manual. When a worn part of the cell needs to be repaired or when new substances need to be produced, genes will give instructions for doing so.
Every cell in our body is surrounded by a fatty membrane, which is filled with thousands of receptors. These receptors receive information from different parts of the body and pass this information into the cell to form / encode new proteins, burn more or less fat, etc. (Note: this is why it’s important to eat good fats and avoid the hydrogenated fats present in most processed foods so that the cell membrane is more permeable to nutrient delivery.) It’s this membrane with receptors the cell command center so if we remove these membrane receptors, the cells die. This means that cell function is highly influenced by external factors, namely through hormones and other molecules that bind to these receptors.
These messenger molecules are not randomly created by our body, they are created according to our lifestyle, diet, thoughts, behaviors, temperature, light, sound and… our type of training. It’s possible to be born with some defective genes – for example BRCA 1 and BRCA 2, which increase the risk for breast cancer – but it’s these messenger molecules / hormones that will determine the degree of activation of these genes. Therefore, controlling these hormones means controlling the body.
(Note: Don’t you find it strange that almost 90% of health care costs is related to treat health conditions, while 80% of health problems / diseases arise as a consequence of our lifestyle and the environment we’re exposed to? Check this TED talk from Dan Buettner to realize why we are walking in the wrong direction).
High-intensity exercise is the one that induces a more favorable hormonal environment, with an increase in hormones such as testosterone, growth hormone and IGF-1, interleukins with an important role in inflammation (IL-6), muscle tissue maintenance (IL-15) and growing of new blood vessels (IL-8), lactic acid (which has the ability to keep us young by stimulating the release of testosterone and growth hormone) and nitric oxide, a vasodilator which plays a key role in regulating blood pressure, muscle strength and erectile dysfunction. Unfortunately, long running does not produce the same effects. Compound movements, which require a combination of strength and stamina, in short periods of time, are those that will put your muscles to “talk” more with your body. Burning calories is only a minor side effect when compared to the amount of hormones and other signaling molecules that influence how our body works.
To be clear, we are talking about intensity coupled with movement quality. Intensity coupled with bad movement will have the opposite effect: INJURY.
Conclusion
It’s urgent to give rise to a new mentality on training the movement skills that we will need throughout our lives. And this is a serious limitation of most group classes in conventional gyms. The instructors are obliged to follow a certain beat and choreography. Individualized feedback is almost non-existent. People don’t have time to understand or to learn the movements. And no one learns anything if they don’t know what it’s for, no one learns anything if they don’t understand how it’s supposed to feel and its practical implications. In addition, most machines in gyms annihilate the sensory and body perception that we, humans, need. We live in a three-dimensional world, in a world of constant adaptation and spatial exploration, so it makes no sense that machines and choreographies of group classes dictate the rules of our movement.
And why is it important to learn efficient movements? First, an efficient movement happens when a body is able to produce force through a coordinated action between the various body segments without energy leaks and demonstrating a natural ability to exploit maximum range of motion. Second, it’s movement that will allow you to play more time with your children, change the furniture at home, improve your day-to-day performance and your performance in your recreational activities.
Look at this type of training as the foundation, the support you need to get stronger, faster, smarter, more agile, more competent in a series of physical attributes that will allow you to perform better in the activities you enjoy doing. Would you like to start playing tennis? golf? volleyball? Would you like to start surfing? paddle board? weightlifting? powerlifting? dance? climbing? triathlon? Would you like to be faster when you play football with your friends during on weekends? Obviously, each modality has its specific abilities, but they all share the same foundation: human being’s adaptability capacity. To improve these specific skills safely, you first need to improve your fundamental movement patterns. And to sustainably keep improving these fundamental movement patterns, you need to train better and respect the developmental stages of each one.
To sum up, the great advantage of better training (and I remind you what we learned about the power of exercise, good movement and a new way of looking at training) is to improve your quality of life, maximize your performance and, above all, giving you the freedom and autonomy to choose the activity / sport that you always wanted to try but never had the courage or opportunity to start off.
Think about these things next time you go to the gym to walk on the treadmill with your headphones on and watch some TV series for 40 minutes while looking at the calories burned on the monitor and at the workouts or exercises other people are doing.
See you soon!
Pedro Correia
References
Berardi, J, Andrews, R. The Essentials of Sport and Exercise Nutrition. Certification Manual. Second Edition. Precision Nutrition Inc. (2013).
Björntorp P. Hormonal control of regional fat distribution. Hum Reprod. 1997 Oct;12 Suppl 1:21-5. Review.
Frederick F. Samaha, M.D., Nayyar Iqbal, M.D., Prakash Seshadri, M.D., Kathryn L. Chicano, C.R.N.P., Denise A. Daily, R.D., Joyce McGrory, C.R.N.P., Terrence Williams, B.S., Monica Williams, B.S., Edward J. Gracely, Ph.D., and Linda Stern, M.D. A Low- Carbohydrate as Compared with a Low-Fat Diet in Severe Obesity. N Engl J Med 2003; 348:2074-2081.
Gary D. Foster, Ph.D., Holly R. Wyatt, M.D., James O. Hill, Ph.D., Brian G. McGuckin, Ed.M., Carrie Brill, B.S., B. Selma Mohammed, M.D., Ph.D., Philippe O. Szapary, M.D., Daniel J. Rader, M.D., Joel S. Edman, D.Sc., and Samuel Klein, M.D. A Randomized Trial of a Low-Carbohydrate Diet for Obesity. N Engl J Med 2003; 348:2082-2090.
Houston, M. What your doctor may not tell you about Heart Disease. Grand Central Life & Style (2012).
Kraemer WJ, Volek JS, Clark KL, Gordon SE, Puhl SM, Koziris LP, McBride JM, Triplett- McBride NT, Putukian M, Newton RU, Häkkinen K, Bush JA, Sebastianelli WJ.
Influence of exercise training on physiological and performance changes with weight loss in men. Med Sci Sports Exerc. 1999 Sep;31(9):1320-9.
Schuenke MD, Mikat RP, McBride JM. Effect of an acute period of resistance exercise on excess post-exercise oxygen consumption: implications for body mass management. Eur J Appl Physiol. 2002 Mar;86(5):411-7. Epub 2002 Jan 29.
Tremblay A, Simoneau JA, Bouchard C. Impact of exercise intensity on body fatness and skeletal muscle metabolism. Metabolism. 1994 Jul;43(7):814-8.
van Gent RN, Siem D, van Middelkoop M, et al Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review British Journal of Sports Medicine 2007;41:469-480.
This is an article on a topic that is very special to me. I’m going to talk about myself, about music, about musicians, about sports and about physical preparation.
I will explain how it is possible to play at the highest level for many, many years in a healthy way and without having to practice endless hours of scales with perfect technique. I will explain how it is possible to avoid tendinitis and other musculoskeletal injuries that typically affect musicians sooner or later, which result from long hours of practice of repetitive gestures in very “unnatural” positions. Yes, it is possible to avoid, mitigate or even eliminate pain in your back, shoulders, neck, elbows, wrists and fingers, which are so common among professional musicians.
Me and music …
Those who have known me for less than 10 years probably don’t know, but I have had a career as a professional musician for at least the previous 10 years. I’ve started playing bass guitar and at a certain point I switched to double bass. I’ve studied at several schools in Portugal (Lisbon Conservatory, Lisbon Superior School of Music and Hot Club of Portugal Jazz School where I would become a teacher) and graduated from the Conservatory of Amsterdam. I was in fact obsessed with playing double bass and particularly obsessed with playing it with perfect technique! I used to practice a reasonable number of hours a day and was able to subject myself to incredibly boring exercises for many hours in a row, just because I wanted to improve a certain aspect of my performance. I could practice about 10 hours a day. For the less familiar with music instruments, the double bass is a very physically demanding instrument, and 10 hours of repetitive gestures in unbalanced positions is very stressful on the body.
Due to long hours of musical practice, I developed a debilitating neuromuscular pathology (focal dystonia) that led me to a long rehabilitation process and to put my music career on hold. To know what focal dystonia is follow this LINK. In addition to focal dystonia, the list of complaints included:
- Frequent back pain, particularly in the lower back;
- Pain and stiffness in the neck, the sensation of having a wry neck that never went away;
- A thoracic kyphosis already up to a non-physiological degree;
- Protruded (forward) shoulders;
- Uneven hips. Because I spent many hours standing leaning mostly over my right leg and in slight lateral flexion, my pelvis was tilted to that side, just like my torso and shoulder. In fact, my right side was all “shortened”, as if I had one leg shorter than the other, which anatomically does not occur;
- Highly rigid and weak wrists, hands and fingers. For instance, I could not hold a push-up position on the floor with arms straight and shoulders over the hands, because my wrists would hurt and did not extend enough.
To aggravate all these imbalances caused by specific and repetitive gestures, my choices for physical activity (yes, because my past in sports impelled me not to be sedentary) relied on activities that were also specific and that also included repetitive gestures, that is, I would play sports! By definition, any sport and its related gestures are specific, cyclic, repetitive and asymmetric. There are sports “less bad” than others, but they are all asymmetrical. And no, swimming is not a complete sport, none is!
All this, and particularly the highly traumatizing and time-consuming process of neuromotor retuning that I underwent to treat dystonia, has prompted me to better understand processes related to the neuromuscular function, motor control, and musculoskeletal injuries. I decided to go back to the university and start a new career, and discovered other obsessions: anatomy, physiology, nutrition, strength training. And here I am today!
Musicians and the myths about “frailty” of their fingers and body …
I have to acknowledge, and my musician friends must forgive me, but musicians are usually very lazy to do any physical activity. We live to play our instruments and to be available for rehearsals. We make up excuses such as not having time and / or that our working tools (e.g. hands and fingers) are very “sensitive” and prone to injury if we engage in any vigorous physical activity. The fear of twisting a finger or cutting a lip (for wind instrumentalists) or even a foot (for drummers) is understandable! In fact, a finger injury for example may be enough to impede a musician from working for several weeks.
Who hasn’t witnessed or lived the situation where when playing soccer with friends those who are musicians try to avoid playing as the goal keeper with fear of injuring their fingers? Perfectly legitimate and understandable. And it’s precisely for this reason that if musicians want to get in better shape and ensure they can play music without injuries for many more years, doing sports is not the solution. They can do it for pleasure, and the energy expenditure that results from it can have positive metabolic effects. However, all asymmetries and musculoskeletal injuries that result from playing an instrument will not be corrected by playing a particular sport and will most likely will be worsened.
Musicians should do general physical preparation instead! Because a professional musician is a highly specialized high-level athlete. A high-level athlete practices his sport and in his training program is (or at least should be) included a very important component which is basic physical preparation. In his physical preparation program our athlete trains for strength, mobility and endurance, and other physical qualities in order to establish a general athletic base that will make him more resilient and protect him from injuries that his sport, which is repetitive and asymmetrical, makes him vulnerable to.
We don’t get fit FROM PLAYING sports, we should get fit TO PLAY sports. The repetition of specific sports gestures induces specific musculoskeletal adaptations. It is easy to understand that for an athlete, it does not make sense to try to compensate for a specific adaptation induced by a sport gesture with another one which might apparently look as an opposite one! For example, will it be smart for a right-handed tennis player to try compensating for the asymmetries resulting from playing with his right arm by engaging in the practice of table tennis with his left arm? Or, if our player exhibits pain in the right shoulder associated with lack of flexibility and strength, does it make sense to start practicing gymnastics just because apparently gymnasts have strong and flexible shoulders? No and no! This athlete should follow a program of general physical preparation to become stronger and more mobile, which can in fact compensate for the asymmetries induced by the sport that he practices.
What is the similarity between playing an instrument and practicing a sport? It’s the same…
Imagine compensating for the unbalanced position of playing double bass with playing another instrument in a seemingly opposite position?
Let’s explore that idea…
For example, playing double bass (a string instrument that can be played with a bow or fingers of the dominant upper limb) implies (usually) standing in a position characterized by unilateral rotation and flexion of the torso, accompanied by a forward leaning of the trunk, in a bipedal position with greater weight over the side of the torso’s lateral flexion, with elevation of both non-dominant arm and shoulder paired with depression of both dominant arm and shoulder, and rotation and slight lateral flexion of the head.
So, to compensate for or correct all these adaptations will it make any sense to go play the violin for example? Because apparently, it’s the opposite! You are (usually) sitting and not standing, the rotation and flexion of the head is in the opposite direction, where both dominant arm and shoulder are apparently more depressed, and the dominant arm raised …? Of course not…
By the same token, this musician will not be stronger, more flexible and more resilient to injuries due to his musical practice if he chooses to compensate for these adaptations with the practice of a sport. If you enjoy playing football or tennis with friends, you should do so, but it will not make you more resilient to injuries or attenuate the ones you may already have.
You must go to the basics: physical preparation.
Musicians should follow physical preparation program such as an athlete. Playing an instrument is highly specific and doing it regularly and long-term will require some specificity and in terms of exercises that can compensate for those unnatural positions that are held for such long periods of time. Yet, the basis of physical preparation will always be (for the athlete, musician, or any other) of a general nature. It is necessary to make the body stronger and more flexible, because only that way one can make it more resilient in order to endure the highly demanding physical requirements of playing a musical instrument for hours, days and years on end.
The pain and discomfort that you my fellow musician feel now, can improve with physical training! Smart training in a controlled environment. A kind of training that can make all the structures of our body stronger and less rigid. A kind of training that promotes a better alignment of the kinetic chain and that enables you to produce force in fundamental movement patterns such as pulling, pushing, lifting objects off the floor, squatting, crawling, walking and jumping.
And no, your body is not fragile! If it hurts, it’s because it’s somehow weak!
Believe me, I’ve been there, done that… ?
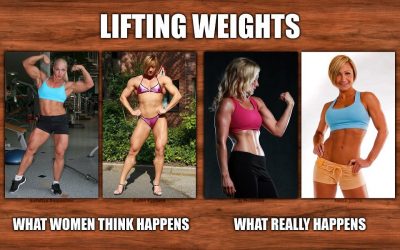
Most women are afraid to lift weights like men because they think they will look bulky and like the women we see on the left hand pictures. It is time to demystify this idea and explain why this is impossible (provided than no hormones and/or anabolic steroids are used), and why strength training is key and a great ally to improve a number of parameters, including body composition.
Overuse of low-intensity training protocols by women is too common. Too much emphasis is placed on cardio, machine use, treadmills, bicycles, light loads, and too little emphasis is put on what will promote better physiological adaptations for increasing women’s functional capacity – strength training. If you want to bring more years into your life, you should start looking at strength training as one of the most effective anti-aging tools on Earth. There is no system in our body that is not influenced by strength training! Have I told you that it is cheaper than the creams you rub on your body every day?
I will divide this article into three parts. First, let’s highlight the myths of strength training for women, which were already addressed by Ebben & Jensen in 1998 in Strengthening for women: debunking myths that block opportunity. Second, let’s highlight its main benefits, and third, let’s explain why you will not look like Arnold Schwarzenegger.
1. MYTHS OF STRENGTH TRAINING FOR WOMEN
- Strength training will cause women to become big and heavy.The truth is that strength training helps to reduce body fat and increase lean mass. These changes may result in a slight increase in weight since the lean mass is more dense than fat (note: if this disturbs you throw the scale away and look more at yourself in the mirror!). Strength training will result in increased strength, no change or a decrease in the hip and waist perimeters and a slight increase in the perimeter of the upper body. Only women who are genetically predisposed for hypertrophy and who participate in high volume and intensity workouts may see substantial increases in the circumference of their limbs.
- Women should use different training methods than men.Women are often encouraged to use machines and to do many repetitions slowly because they are afraid that the use of free weights, manual resistance, explosive movements or exercises that use their body weight as resistance will cause injury. In fact, there is no evidence suggesting that women are more likely than men to injure themselves during strength training. The most important factors to reduce the risk of injury are based on exercise technique and training individualization.
- Women should avoid high intensity training or training with high loads.Women are usually encouraged to use smaller weights in their strength training (i.e., light dumbbells) but the problem is that these light loads are substantially below what is required to promote physiological adaptations. Women need to train at intensities high enough to promote adaptations in bones, muscles, cartilage, ligaments and tendons. When the intensity of the exercise is low, that is, when the stimulus is insufficient, the physiological benefits are minimal. To maximize the benefits of strength training, women should train close to their maximum. For women who have had children, imagine that this is what you have to “push” to get the greatest benefits.In short, there is no reason for women to train differently from men with regard to training intensity. If you intend to get different results, you need to leave aerobic classes and pink weights to start lifting real weights.
2. STRENGTH TRAINING BENEFITS FOR WOMEN
In addition to improving body composition (loss of fat mass and increase in lean body mass), strength training will help you:
- Increase bone remodeling. You will get stronger bones and reduce the risk of osteoporosis (LINK, LINK, LINK). Keep in mind that stronger bones can also result in total weight gain, but this is good, strong bones are a sign of health;
- Strengthen the connective tissue. You will increase your joint stability and reduce the risk of injury (LINK). As in the previous point, same thing can happen regarding weight gain;
- Increase functional strength for activities you enjoy or for your daily activities (e.g. playing with your kids, carrying grocery shopping, climbing stairs).
- Increase self-esteem and confidence. A stronger body will make your mind stronger and unstoppable!
- Fight the effects of metabolic syndrome and other common chronic diseases in our society, such as cardiovascular disease, type II diabetes, cancer, fibromyalgia, rheumatoid arthritis and Alzheimer’s disease (LINK, LINK).
- Increase longevity in a healthy way. Strength training will potentiate the release of anabolic hormones that play an important role in tissue regeneration and anti- aging (LINK).
In summary, strength training has the potential to restore the shape of your glutes, the glow of your skin and the tonus of those parts of the body that you think is only possible through surgery, miracle supplements and advanced techniques of “muscle toning”. Strength training can also help you live the life of your dreams.
3. WHY I WILL NOT BECOME ARNOLD SCHWARZENEGGER?
Women have different physiological characteristics from men and this is the reason why women have greater difficulty in gaining muscle than men. As I said at the beginning of this article, if there are no hormones and/or anabolic steroids involved, it is very unlikely that women will look like men.
- Diferences in muscle fibersAlthough women have the same types of muscle fibers that men have (fast-twitch fibers and slow-twitch fibers), the amount of muscle fibers they have and their size is smaller. Remember that slow-twitch fibers (type I) are used primarily in endurance efforts whereas fast-twitch fibers (type II) are used primarily in rapid and explosive movements. In women, because they have 70-75% type I fibers, it becomes even more difficult to move loads at high speeds. This means that the potential for increasing the cross-sectional area of the muscle (i.e. muscle size) and for increasing the rate of force development is lower in females than in males.
- Diferences in strength and powerThe average total body strength of a woman corresponds to about 60% of the average total body strength of a man. In average, upper body strength in women ranges from 25-55% of men’s upper body strength. Regarding lower body strength, it seems that women are stronger in relative terms. In average their capacity is 70-75% of what is observed in men. It is therefore not surprising that most women find it more difficult to lift weights with arms and upper body (e.g. push-ups and pull-ups) than with legs and lower body (e.g. squats and lunges).
- Diferences in hormone levelsThe most obvious difference in the mechanisms that determine the adaptations to training of men and women is the sex hormone, testosterone. Both men and women produce testosterone, the difference is that testosterone concentrations in men are 10 to 20 times higher than in women! It appears that women are more dependent on pituitary secretion from growth hormone and other growth factors to help mediate changes in muscle, bone and connective tissue. In fact, although strength training adaptations do not occur in the same way, it has been reported that women have higher bioavailable concentrations of growth hormone at rest than men. Fortunately, strength training and metabolic resistance training can also increase growth hormone levels.Also, if you begin to lift weights in a progressive manner, you will continue to maintain your femininity, you will not grow a mustache, beard or hair in your chest. You will not get bigger or full of muscles. On the contrary, you will get leaner, stronger, younger, smarter and much more attractive to the opposite sex. But do not be fooled, to get the greatest benefits in training, you need to work hard and realize that it takes serious effort to induce the metabolic adaptations you seek (e.g. improving body composition and biological aging). This does not happen overnight. You will need time, consistency and discipline. There are no miracle pills.
In conclusion, before beginning a strength training program, be aware that you must have movement competency in the first place. Just as you would not begin to calculate derivatives in mathematics before you know how to add and subtract, it also makes no sense to start lifting heavy loads if you have restrictions and/or asymmetries in your movement profile. The quality of movement is the foundational support for functional strength development so this “ingredient” will always have to come first.
For a graphic resource check out this nice infographic from Positive Health Wellness.
See you soon and enjoy 🙂
Pedro Correia
References
Ciccolo Joseph T, Carr Lucas J, Krupel Katie L, Longval Jaime L. The Role of Resistance Training in the Prevention and Treatment of Chronic Disease. American Journal of Lifestyle Medicine July/August 2010 vol. 4 no. 4 293-308.
Cussler EC, Lohman TG, Going SB, Houtkooper LB, Metcalfe LL, Flint-Wagner HG, Harris RB, Teixeira PJ. Weight lifted in strength training predicts bone change in postmenopausal women. Med Sci Sports Exerc. 2003 Jan;35(1):10-7.
Ebben WP, Jensen RL. Strength training for women: debunking myths that block opportunity. Phys Sportsmed. 1998 May;26(5):86-97. doi: 10.3810/psm.1998.05.1020.
Hurley BF, Hanson ED, Sheaff AK. Strength training as a countermeasure to aging muscle and chronic disease. Sports Med. 2011 Apr 1;41(4):289-306. doi: 10.2165/11585920-000000000-00000.
Kraemer WJ, Ratamess NA. Hormonal responses and adaptations to resistance exercise and training. Sports Med. 2005;35(4):339-61.
Nickols-Richardson SM, Miller LE, Wootten DF, Ramp WK, Herbert WG. Concentric and eccentric isokinetic resistance training similarly increases muscular strength, fat-free soft tissue mass, and specific bone mineral measurements in young women. Osteoporos Int. 2007 Jun;18(6):789-96. Epub 2007 Jan 31.
Stone MH. Implications for connective tissue and bone alterations resulting from resistance exercise training. PubMed PMID: 3057317.
Winters KM, Snow CM. Detraining reverses positive effects of exercise on the musculoskeletal system in premenopausal women. J Bone Miner Res. 2000 Dec; 15(12):2495-503.
Zatsiorsky V., Kraemer, W. Science and Practice of Strength Training 2nd Edition. Human Kinetics (2006).
If your grandfather is a normal person, it is very likely that he has been to the doctor many times, that he is on medication, that he does not hear very well and that he does not have the same locomotion capacity and reasoning that he had some years ago.
Doctors say this is “normal” and typical of the advancing age. They also prescribe drugs based on the belief that this will improve the quality of life of these people. I do not say that this is not necessary in some cases, but I do not believe that this is the best approach to increase health span. Although they “breathe” I think that they deserve better and more.
More than two years ago, a piece in a portuguese newspaper stated that the Portuguese lived longer and longer but less healthy. The piece also mentioned: “Portuguese women have one of the longest life expectancy in the world, but, paradoxically, enjoy far fewer healthy years than women from the best-ranked countries in Europe.”
When reading the piece, the first thing I thought was: we have to be really stupid, because even with the daily advances of medicine and scientific knowledge, we have not yet been able to understand what are the causes behind this SICK LONGEVITY. The problem is not the advancing years, the problem lies in nutrition and exercise related advice we hear every day (especially in hospitals), which is simply erroneous. If prevention campaigns and the information leaflets in hospitals were really supported by scientific evidence, one would not witness so many people suffering from chronic pain, diabetes, heart disease, osteoporosis, sarcopenia, autoimmune diseases and cancer.
Everyone recognizes that physical exercise is key to optimal body function (our brain and body did not develop while sitting on our asses), and that, unlike drugs, has a positive and self-regulating impact on the various systems of the human body.
Exercising is more effective on improving your health than any patented medicine.
“But I walk an hour every day”
Let me tell you one thing, walking is the least you can do to keep your body working. If you tell me that is either walking or lying back on the couch eating ice cream, then you better walk. But if you tell me that you want to live a healthy life until you die, maintain your autonomy, decrease the risk of falls, increase self-confidence, sleep better, recover faster from an injury and not be part of the statistics we saw above, then I recommend you start seriously thinking about lifting weights and engaging in strength training. Walking will not give you, even by shadows, the same benefits as strength training.
Another thing, if you are one of those people with cardiovascular disease, your doctor (or some Dr. from Google) has probably told you that walking is important to improve your cardiovascular health. The problem is that walking will not help you much. The lack of aerobic capacity is not a risk factor for heart disease, a sedentary lifestyle is! This means that you may have a huge aerobic capacity and a heart disease at the same time. In fact, according to this study published in the 2006 American Heart Association Journal (LINK), to this one published in 2008 in the European Heart Journal (LINK) and to this one published in the Mayo Clinic Proceedings (LINK) in 2012, marathoners are those who appear to be at increased risk of developing cardiovascular disease.
Furthermore, according to the cardiologist Henry A. Solomon in the book “The Exercise Myth”, cardiovascular health refers to the absence of heart and blood vessel disease, and not to an individual’s ability to do a certain amount of physical work. According to Dr. Solomon, your cardiac health is determined by the condition of various structures of the heart, including the heart muscle, the valves, the special cardiac tissues that carry electrical impulses and the coronary arteries. So, do not expect exercise to “clean” what you practice in your daily diet.
The cardio craze came about in the late 60’s / early 70’s through Dr. Kenneth Cooper, the person who designed the Cooper test for US military use. It was roughly from this moment on that VO2max (a measure of aerobic capacity) was “elected” the holy grail of physical fitness. Although relevant for performance and longevity, VO2max is not the only marker of physical fitness. Strength in its various forms has been more strongly correlated with increased longevity than VO2max. While strength training can increase both functional strength and aerobic capacity, the typical cardio training will not make you stronger and will only slightly “at best” increase your VO2max.
Why Strength Training?
Because you tend to lose strength and power as you age, and because several studies have shown that loss of strength and muscle mass are associated with increased mortality (LINK, LINK, LINK). Fortunately, lifting weights is the best stimulus to counteract this trend and to increase our functional capacity. Under normal conditions, strength peaks between the ages of 20 and 30, remaining relatively stable or decreasing slightly over the following 20 years. But this is dependent, of course, of what one does in training.
It is in the sixth decade of life that decreases in strength are quite pronounced. According to several longitudinal studies, declines in muscle strength are around 15% between 60-70 years of age and 30% after age 70. Most reasons relate to the loss of muscle mass, pronounced loss of fast-twitch muscle fibers, decreased endocrine function, loss of tissue mobility / elasticity and cell dehydration. All of these can be minimized by following a proper strength training program.
Yes, it is possible to start strength training at any age, I know people who started training at 50, 60 and over 80, it’s all a matter of mindset and willpower. Also, you need to train according to your needs as opposed to the convenience of most gyms (i.e. spending hours on the treadmill / elliptical / bike, going through all the machines and ignore training with free weights) where supervision, tutoring and skill learning are dismissed.
Does this mean that I should get my grandparents to lift Olympic bars and weights without any criteria? Of course not, that would not be very smart. To get the most benefit of lifting weights you have to walk a path and create a solid movement base. You have to be screened and assessed for movement quality and physical parameters. Preferably guided by a fitness professional or personal trainer knowledgeable in movement and strength training science.
Listen, your doctor’s opinion might be highly valuable, however remember the following: 1) your doctor is not a specialist in movement (which is ok, they can not be trained in everything); 2) your doctor has no experience training people (which is also ok, it’s not their job); 3) your doctor probably does not even know how to lift weights or to move well (this is obviously not ok!). In other words, just as you would not ask advice on surgery techniques from strength coaches, you should also not ask advice on training methodologies and forms of physical exercise from surgeons.
Oh, and before you tell me that I’m being fundamentalist and suggesting that you should not train other physical abilities (such as stability, mobility, endurance, speed, agility, motor coordination, power), allow me to conclude with the following observation: ideally, the training program of any human being on the planet should always be the one that induces the adaptations necessary to fulfill his /her personal goals.
The key word here is adaptation! The more adapted you are the better prepared you will be to face any situation. Adults are free to do whatever they want in life. Everyday we make decisions and choices and those decisions matter. My goal is to increase longevity and live until the last days of my life feeling great and strong.
What’s yours?
See you soon!
Pedro Correia
References
Möhlenkamp S, Lehmann N, Breuckmann F, Bröcker-Preuss M, Nassenstein K, Halle M, Budde T, Mann K, Barkhausen J, Heusch G, Jöckel KH, Erbel R; Marathon Study Investigators; Heinz Nixdorf Recall Study Investigators. Running: the risk of coronary events : Prevalence and prognostic relevance of coronary atherosclerosis in marathon runners. Eur Heart J. 2008 Aug;29(15):1903-10. doi: 10.1093/eurheartj/ehn163. Epub 2008 Apr 21.
Neilan TG1, Januzzi JL, Lee-Lewandrowski E, Ton-Nu TT, Yoerger DM, Jassal DS, Lewandrowski KB, Siegel AJ, Marshall JE, Douglas PS, Lawlor D, Picard MH, Wood MJ. Myocardial injury and ventricular dysfunction related to training levels among nonelite participants in the Boston marathon. Circulation. 2006 Nov 28;114(22): 2325-33. Epub 2006 Nov 13.
O’Keefe JH, Patil HR, Lavie CJ, Magalski A, Vogel RA, McCullough PA. Potential adverse cardiovascular effects from excessive endurance exercise. Mayo Clin Proc. 2012 Jun;87(6):587-95. doi: 10.1016/j.mayocp.2012.04.005.
Rantanen T, Harris T, Leveille SG, Visser M, Foley D, Masaki K, Guralnik JM. Muscle strength and body mass index as long-term predictors of mortality in initially healthy men. J Gerontol A Biol Sci Med Sci. 2000 Mar;55(3):M168-73.
Ruiz JR, Sui X, Lobelo F, Morrow JR Jr, Jackson AW, Sjöström M, Blair SN. Association between muscular strength and mortality in men: prospective cohort study. BMJ. 2008 Jul 1;337:a439. doi: 10.1136/bmj.a439.
Takata Y, Ansai T, Soh I, Akifusa S, Sonoki K, Fujisawa K, Awano S, Kagiyama S, Hamasaki T, Nakamichi I, Yoshida A, Takehara T. Association between body mass index and mortality in an 80-year-old population. J Am Geriatr Soc. 2007 Jun;55(6):913-7.
Zatsiorsky V., Kraemer, W. Science and Practice of Strength Training 2nd Edition.
Human Kinetics (2006).

Several lines of evidence suggests that mitochondrial dysfunction is associated with sarcopenia (loss of strength and muscle mass in aging). In every cell of our body there are hundreds or thousands of mitochondria, they exist in greater quantity in the most active organs and tissues (muscles, heart and brain). The reason we age faster derives from the constant injuries and insults inflicted to the mitochondria. Chronic stress, lack of sleep, poor eating choices, lack of exercise (particularly strength training), alcohol, tobacco, and exposure to pollutants are just a few examples of how our lifestyle can influence the function of these small structures.
Mitochondria are the organelles responsible for energy production in our body. If you feel always tired, if you experience memory loss, if you have frequent muscle pain and if you are one of those people taking medications for cholesterol, hypertension, diabetes and other chronic diseases, it is very likely that your mitochondria are not in “great shape”. But let’s look at some evidence.
This study may be considered revolutionary because of its highly relevant findings regarding the benefits of strength training in older people. This study was published in 2007 and was the first study human study to demonstrate that strength training can reverse the aging process at molecular level. If it was a drug or a food supplement demonstrating these effects, I think everyone already knew.
Sample
The researchers recruited 25 healthy elderly people (mean age 68 years), who already did some type of physical exercise (walking, gardening, tennis, golf, cycling) three to four times a week, and 26 young adults (mean age 24 years) relatively inactive, some of them participating in recreational activities.
The authors selected relatively active older adults and sedentary young adults in order to study the aging process on healthy elderly and not just the putative aging effect of physical inactivity. All older subjects underwent a thorough screening process before being admitted to the study to ensure that other factors (e.g. metabolic diseases) would alter mitochondrial function.
All subjects completed a medical evaluation before participating in the study. Exclusion criteria were: evidence of heart disease (by history and sub-maximal graded exercise test); hypertension; chronic obstructive pulmonary disease; diabetes mellitus; renal insufficiency; orthopedic injury and smoking. None of the subjects had previously participated in a structured resistance training program.
Training Program
Subjects performed resistance exercises with supervision on two nonconsecutive days of the week (monday/thursday or tuesday/friday) for 26 weeks (six months). The subjects performed twelve different exercises including chest press, leg press, leg extension, leg flexion, shoulder press, lat pull-down, seated row, calf raises, crunches, back extensions, bicep curl and triceps extension.
Subjects initially started with a set of 50% of 1 maximal repetition (1RM), and gradually increased to three sets at 80% of their 1RM during the intervention period. Subjects tested their 1RM for every exercise every two weeks, and training loads were adjusted to maintain 80% of their 1RM.
Muscular Biopsy
All younger subjects (N = 26) underwent a muscle biopsy (incision and extraction of a small part of muscle) from the vastus lateralis (thigh muscle) before and after the 26-week study. The elderly subjects (= 25) did their biopsies before the study and after (N = 14) of the study. Muscle RNA (ribonucleic acid) was analyzed to determine age-related gene expression variation.
Results
The authors identified 596 genes that were differentially expressed between the two age groups. Of the 596 genes, the researchers identified 179 associated with age and exercise that showed a remarkable reversal in their expression profile after six months of resistance training. This literally means that resistance training not only can slow down but also reverse the aging process at the genetic level. The genetic expression of the elderly individuals became similar to those of the younger group. The researchers also noted that mitochondrial dysfunction (closely related to physical inactivity) began to reverse after six months of training.
As for muscular strength, results were as expected, that is, the ones who strength trained got stronger. The initial gap of 59% in maximal isometric strength in older people vs. young adults was reduced to 38% after six months of resistance training.
Conclusions
Nowadays, it is widely accepted that physical exercise is associated with a decrease in morbidity and mortality in humans. This is not a belief. What people probably do not know is that there are forms of physical exercise that are more effective in increasing strength and longevity. This study demonstrated for the first time that resistance training can reverse age-related aspects at the gene level. Yes, you are reading well, resistance training can reverse aging at the molecular level!
The fact that older people got stronger was no surprise to me and certainly not for fitness professionals. It is not uncommon for older people to begin their training with minimum weights and, in a short time, evolve to loads equal to or greater than those in their twenties. It’s all about dedication, consistency and method.
Over the years, personal trainers and fitness professionals have been preaching their clients / athletes about the importance of physical exercise in improving health. This message, in my opinion, has not been well perceived by most people. Understanding the notion that movement and physical exercise is as important as the food they eat every day is, unfortunately, still lacking.
In short, this fascinating study is basically telling us that it is within our power to increase health and longevity. In this case, the “fountain of youth” is something we know and something that is relatively accessible to everyone – Strength Training.
However, for these benefits to occur, people have to be willing to work hard and with consistent effort, something rare in our “all in moderation” oriented society. Most people are in search of a miraculous pill and rather rely on faith than doing something for themselves. Therefore, I believe that only focused individuals and those who follow these principles in training (and in life) will end up having the most benefits. Things will not happen by chance, certainly.
See you soon!
Pedro Correia
References
Melov S, Tarnopolsky MA, Beckman K, Felkey K, Hubbard A (2007) Resistance Exercise Reverses Aging in Human Skeletal Muscle. PLoSONE 2(5): e465. doi:10.1371/ journal.pone.0000465

The Swing exercise is the foundation of hardstyle kettlebell training methodology and an essential exercise in our training programs at The Strength Clinic. The hardstyle Swing is an explosive movement characterized by a vigorous and complete extension of the knees and hips (in the top position) preceded by near maximal hip flexion and slight knee flexion (in the bottom position). The Swing is known for its effectiveness in improving performance in daily life activities as well as performance of athletes of the most varied modalities, from long distance runners to combat sports, among others. We can point out five reasons that make the hardstyle kettlebell Swing an exercise of choice for athletic development:
- Strength. The acceleration and deceleration component inherent to the Swing induces important adaptations in the power production capacity despite the relatively light loads used. Reminding Newton’s second law (force = mass x acceleration), it is possible to increase force acting on a given system by increasing acceleration without increasing mass. In this case, the real load manipulated during some moments of the Swing performance will exceed the weight in Kg of the kettlebell, where peak forces generated can be up to 10 times more. This allows for significant maximal strength gains especially in the posterior chain;
- Power. Due to its explosive nature based on a fundamental movement pattern (i.e. “hip hinge”, used in deadlift exercise). The vigorous extension of the hips and knees is at the base of any explosive athletic movement. The Swing not only allows you to work explosive strength, but also allows you to do it in a cyclical and repetitive way, and also in a very safe way. This feature constitutes an advantage of the kettlebell Swing in terms of benefit / risk, when compared to the Olympic movements like the Snatch or the Clean for power development. The Swing is not only less technically complex to learn, it allows greater number of repetitions without fatigue compromising (in a dangerous way) technical execution;
- Trunk stability and rotational strength. The biofeedback offered by holding a kettlebell and the need to balance the forces generated by the acceleration and deceleration of the kettlebell, induces a marked activation of the stabilizing muscles of the trunk and shoulder joints. When performed with one hand, the Swing further accentuates muscle activation in a crossed chain fashion due to the anti-rotational component created. This type of rotational power generation manifests itself in the most varied sports movements, such as: the golf swing; the serve, forehand and backhand stroke in tennis; shooting in handball; shooting and serve in volleyball; shooting and kicking in soccer; throwing events in track and field athletics; etc;
- Muscle and cardiovascular endurance. Due to its particular design, the kettlebell Swing allows repetition of explosive movements with maximum or near maximum acceleration. This possibility of safe repetition with an additional load delivers significant muscle and cardiovascular endurance adaptations;
- Fat loss. Because it entails the stimulation of large amounts of muscle mass at a high intensity and repetitive way, the kettlebell Swing induces high metabolic stress levels. This metabolic stress results in increased oxygen consumption in the subsequent hours (i.e., increased calorie expenditure due to increased metabolism), thus contributing greatly for fat loss.
Indeed, the inclusion of the kettelbell Swing is a wise choice when structuring a well-rounded training program. The Swing is also highly versatile in terms of programming. By combining different loads, number of repetitions, rest periods and variations of the exercise (e.g. two-handed Swings, one-handed Swings, double Swings, dead stop Swings), one can easily shift the pointer in order to work on specific adaptations of the strength continuum (i.e. from the maximum strength end to the muscular endurance end) as well as on the various energy systems. And all this in a very safe way!
A 12-week fat loss program suggestion
Get a kettlebell (at least 16kg for women and 20kg for men) and have it in your living room or bedroom. Learn how to perform the hardstyle swing exercise with a certified instructor. Every day, whether you train in the gym or not, perform 5 sets (spread throughout the day according to your own convenience) of 20 swings during the first week, 25 swings during the second week, 30 swings during the third week and 35 swings during the fourth week. On the second month repeat the process with a kettlebell at least 4kg heavier, and on the third month with a kettlebell 8kg heavier. At the end of 12 weeks rejoice with the results!
Swing and enjoy…! 🙂
Nuno Correia